



North America's healthcare automation market is estimated at USD 42.91 billion in 2025 and projected to reach USD 104.41 billion by 2035, growing at a 9.30% CAGR from 2026 to 2035, according to Towards Healthcare market insights on healthcare automation. For a Canadian hospital board, that number isn't just a market signal. It's a sign that automation has moved from optional improvement to operating model.
The harder truth is that many organisations still talk about automation as if it means buying a bot, adding a portal, or sending appointment reminders. That's too narrow. Good healthcare automation solutions change how work moves across the hospital. Great ones reduce friction for staff, shorten delays for patients, and support safer decisions without turning clinicians into screen managers.
In Canada, that distinction matters. Hospitals and clinics are trying to handle workforce pressure, rising demand, compliance obligations, fragmented data, and growing expectations around digital care. If automation only speeds up paperwork, it helps a little. If it reshapes work around people, it can relieve some of the pressure that is driving burnout in the first place.
The Urgent Case for Healthcare Automation in Canada
Canada is not approaching healthcare automation as a side project. It has already been framed as part of a broader national response to workforce shortages and population growth. A Canadian government research effort concluded that technology is advancing rapidly and that innovations such as robotics, artificial intelligence, and 3D printing are essential to addressing doctor and nurse shortages through automation, as discussed in this analysis of Canada's healthcare automation direction.
That same work led the Canadian Senate to recommend a Forum for Health Discovery, a National Conference on Robotics, Artificial Intelligence and 3D Printing in Healthcare, and dedicated working groups to address technological, ethical, and regulatory questions. Those recommendations matter because they show automation isn't only a procurement issue. It's a governance issue, a workforce issue, and a care delivery issue.
Why boards should treat this as a strategic decision
A board usually asks three questions: why now, where is the pressure strongest, and what happens if we wait?
The pressure points are familiar:
Workforce constraints: Clinical and administrative teams are carrying heavy repetitive workloads.
System fragmentation: Patient, billing, supply, and diagnostic systems often operate in silos.
Rising complexity: More digital tools can either simplify work or make it harder, depending on implementation.
Board-level test: If your clinicians still re-enter the same information into multiple systems, your organisation has an automation problem, not just a staffing problem.
Waiting has a cost even when it doesn't show up clearly in a budget line. Delayed handoffs, duplicate entry, manual verification, inventory blind spots, and billing backlogs all consume staff attention. In healthcare, attention is one of the most expensive resources you have.
Automation as infrastructure, not gadgetry
Some organisations still evaluate healthcare automation solutions as isolated tools. A claims bot here. A scheduling workflow there. That approach can create local wins, but it rarely fixes the full patient and staff journey.
A better view is to treat automation like hospital infrastructure. You don't buy a lift because it's fashionable. You buy it because a building can't function well without reliable movement between floors. Automation plays a similar role for digital work. It moves information, tasks, alerts, approvals, and decisions to the right place with less manual chasing.
That is why this has become urgent. In Canada, the conversation has already moved beyond “should we automate” to “how do we integrate automation responsibly into care.”
Decoding Healthcare Automation Beyond the Buzzwords
Most confusion starts with the word “automation” itself. People hear it and think of robots replacing humans. In practice, healthcare automation solutions are usually better understood as work coordinators. They don't remove the need for people. They reduce the amount of low-value effort people spend moving information around.
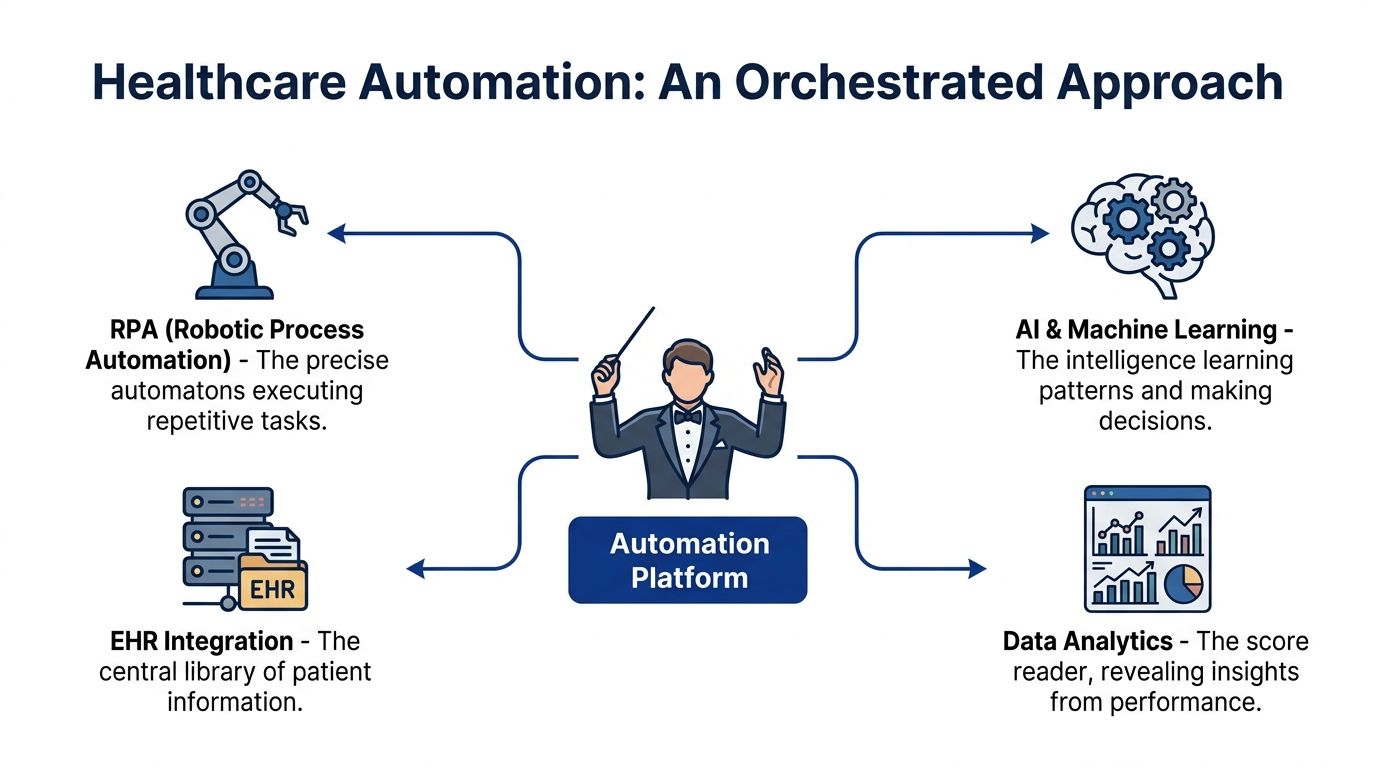
A useful analogy is an orchestra. In a hospital, registration, clinical documentation, pharmacy, billing, lab systems, and inventory all play different instruments. If each one performs well on its own but never follows the same score, the result is noise. The automation platform acts like the conductor. It cues the right action, at the right moment, in the right system.
What automation actually does in daily operations
At the simplest level, automation follows defined rules. If a referral arrives, route it. If an insurance field is missing, flag it. If a lab result crosses a threshold, notify the responsible team.
At a more advanced level, automation can interpret inputs, prioritise work, and support decisions. That's where AI enters. It can read unstructured text, recognise patterns, classify documents, suggest next steps, or help staff focus on the highest-priority cases first.
A plain-language breakdown helps:
| Type | What it does | Hospital example |
|---|---|---|
| Rule-based automation | Follows pre-set instructions | Sends appointment reminders or routes a completed form |
| Workflow automation | Moves tasks between people and systems | Escalates a discharge task when pharmacy approval is complete |
| AI-enabled automation | Interprets messy information and supports decisions | Reads scanned forms and maps key details into records |
The difference between isolated tools and orchestrated systems
Many hospitals already have automated features buried inside existing software. That doesn't mean they have a coherent automation strategy. A reminder system, an e-form, and a billing macro can each work, but still leave staff switching screens and repeating tasks.
That's why the “conductor” idea matters. Real value comes from connection:
Admin workflows connect to clinical workflows: Intake details reach the chart without re-entry.
Clinical workflows connect to revenue workflows: Documentation supports coding and claims preparation.
Supply workflows connect to care workflows: Staff can locate equipment and medication faster.
A hospital doesn't need more isolated automation. It needs fewer gaps between systems.
When readers get confused, it's often because vendors mix up task automation with operational redesign. Task automation speeds up one step. Operational redesign changes how the whole process works. Boards should ask for both viewpoints before approving any investment.
The Core Technologies Driving Automation
The market uses a lot of labels, but most healthcare automation solutions are built from a manageable set of technologies. If you understand the role of each one, vendor conversations become much easier.

Robotic process automation
Robotic Process Automation (RPA) is software that handles repetitive digital tasks by following defined steps across applications.
Think of RPA as a careful clerk that never gets bored. It can open systems, copy values, check fields, trigger updates, and move forms from one queue to another. In healthcare, that often means registration checks, referral routing, prior authorisation support, or status updates in legacy systems that don't integrate neatly.
A relatable example is eligibility verification. Instead of asking staff to log in to multiple payer or internal systems for every patient, an RPA bot can collect those checks and present the result for human review.
EHR and EMR automation
EHR and EMR automation reduces manual chart work by moving data into the right record fields and triggering actions from documented events.
The implementation of automation often determines whether many organisations gain clinician trust or lose it. If automation improves chart completeness without forcing extra clicks, staff adopt it. If it adds alerts, duplicate fields, or awkward templates, resistance rises quickly.
Document ingestion is a practical example. Scanned referrals, handwritten notes, and external forms can be read and mapped into structured fields rather than manually retyped. That's also why many teams look closely at tools for speech and note capture. If you're reviewing options for documentation workflows, this guide to choosing medical voice recognition vendors is useful because it highlights selection criteria that affect daily clinician experience.
Clinical workflow automation
Clinical workflow automation coordinates time-sensitive actions around patient care tasks.
Its role is less about data entry and more about sequence. Who needs to know what, and when. A strong system can route abnormal findings, prompt follow-up steps, or ensure discharge activities happen in the right order.
One example is a critical result pathway. A lab result enters the system, the platform checks the threshold, alerts the designated clinician, records acknowledgement, and escalates if no response arrives within the defined workflow window. That reduces the chance that important information sits unseen in a queue.
AI-driven triage and decision support
AI-driven triage helps classify and prioritise cases based on incoming information rather than only fixed rules.
This matters when volume is high, and inputs are messy. Symptoms described in free text, referral letters, scanned notes, and wearable data don't fit neatly into checkbox workflows. AI can help sort and structure that information so teams can decide faster.
In some healthtech builds, this capability sits inside broader integration work. The practical challenge is connecting models, interfaces, and governance without breaking clinical workflows. For teams evaluating the platform side of this problem, AI integration in healthtech platforms is a helpful technical reference.
Intelligent billing and revenue automation
Intelligent billing automation uses document extraction, language processing, and workflow logic to accelerate the journey from care delivered to claim submitted.
In simple terms, it turns messy administrative material into billable, reviewable data. That can include extracting fields from notes, matching them to billing systems, flagging missing information, and sending work to the right queue. Cleffex Digital Ltd is one example of a provider that builds workflow and AI integrations for healthcare operations, including automation around scheduling and administrative processes.
These five categories overlap, but they don't do the same job. A board that treats them as interchangeable usually buys the wrong tool. The right question isn't “Do we want automation?” It's “Which part of the workflow needs intelligence, which part needs orchestration, and which part just needs reliable execution?”
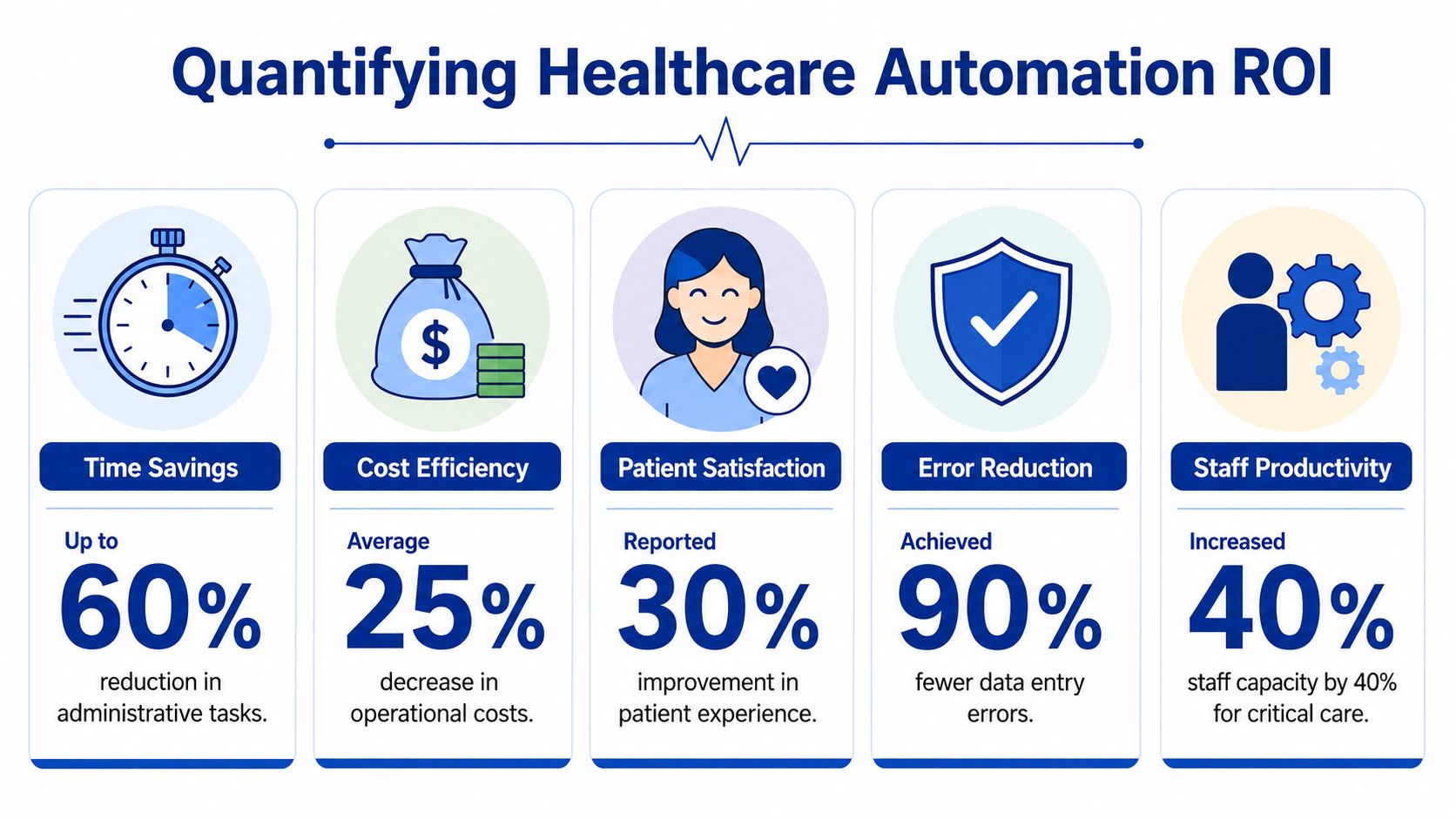
Real-World Benefits and Measuring ROI
Return on investment gets discussed too vaguely in healthcare. “Efficiency” sounds positive, but boards need a sharper lens. The useful question is this: where does automation release staff time, reduce avoidable cost, or improve the reliability of care-critical operations?
The strongest case often starts in the revenue cycle and supply chain because the mechanisms are visible. In the Canadian context, automation tools using NLP with Generative AI are benchmarked to free up nearly 50% of a revenue cycle professional's time by automating front-end tasks such as pre-authorisation and financial clearance, as well as back-end claims processing and collections, according to NetSuite's overview of healthcare automation.
Where measurable value shows up first
That “nearly 50%” figure becomes easier to understand when you picture the work involved. Staff often handle scanned forms, payer documentation, referral notes, and billing support documents that arrive in inconsistent formats. Automation extracts the relevant details, recognises text patterns, and maps them into software fields. That cuts retyping, reduces manual entry errors, and shortens billing latency.
Supply chain automation offers another concrete line of sight. Robotic material handling systems and Automated Storage and Retrieval Systems can reduce operational costs by 20% to 30% in hospital networks through optimised inventory management, according to Dematic's healthcare automation overview. The practical mechanism is simple. “Goods-to-person” workstations bring the item to the worker instead of making staff search shelves, bins, or rooms.
A finance committee can understand both examples because the workflow is tangible:
Revenue cycle: Less manual correction, faster processing, fewer avoidable delays.
Inventory management: Better traceability, less wasted motion, more reliable access to supplies.
Equipment readiness: Predictive approaches can support maintenance and availability planning.
ROI isn't only about finance
Hospitals make a mistake when they stop the analysis at direct savings. Some of the most important returns show up in reliability and staff experience.
Consider the difference between a nurse hunting for a missing infusion pump and a nurse retrieving the right item through a more visible, traceable system. The second scenario isn't only more efficient. It lowers frustration, reduces interruption, and supports faster care. The same applies when billing staff spend less time deciphering documents and more time resolving exceptions that require judgement.
Practical lens: If automation removes routine work but adds mental clutter, the ROI is weaker than it looks on paper.
That's why many boards now review ROI across four categories:
| ROI category | What to look for |
|---|---|
| Time released | Fewer hours spent on repetitive handling and re-entry |
| Cost avoided | Lower operational waste and fewer process bottlenecks |
| Clinical reliability | More consistent handoffs, visibility, and escalation |
| Workforce impact | Less frustration, fewer interruptions, better role focus |
For leaders building the financial case around claims and back-office operations, this explainer on revenue cycle management automation is a useful companion read because it translates operational concepts into boardroom language.
The best ROI stories in healthcare rarely come from one flashy tool. They come from removing friction in places where staff repeat the same effort all day.
A Human-Centred Implementation Roadmap
Many automation projects fail for a predictable reason. They optimise the process map and ignore the person doing the work. In healthcare, that creates a dangerous pattern. A tool reduces one form of effort, then adds interruptions, alerts, screen switching, or mistrust.
Research from the University of Toronto emphasises the need for human-centred automation design to ease stress on overburdened healthcare systems, as explained in the University of Toronto discussion on human-centred automation tools. That idea should shape implementation from the first workshop, not be added later as a change-management exercise.
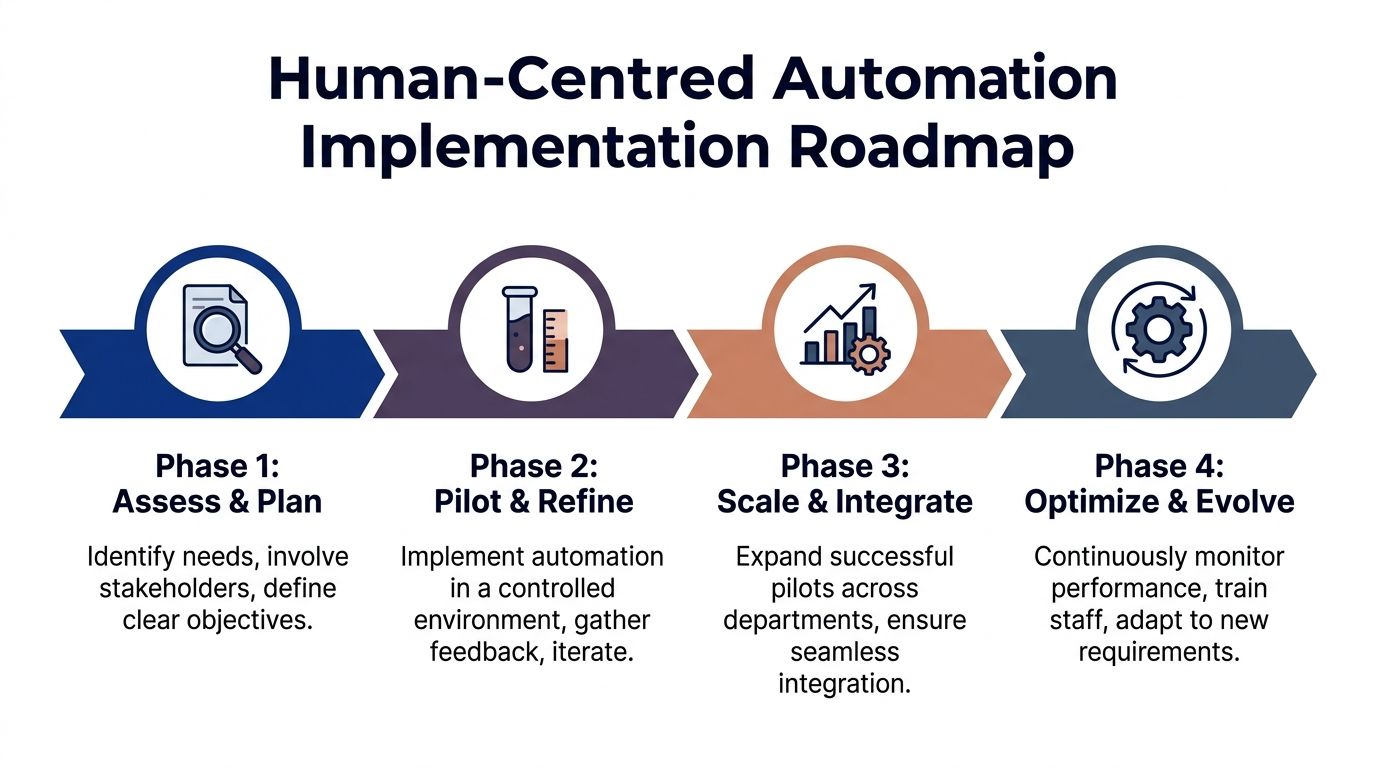
Phase one with the right starting point
Don't begin by asking which technology to buy. Start by identifying where staff lose time, attention, or confidence.
A short assessment should examine:
Rework hotspots: Where information gets re-entered or corrected repeatedly.
Delay points: Where tasks wait because ownership is unclear.
Stress points: Where clinicians and admin staff report interruptions, queue overload, or alert fatigue.
This is also the stage to map who touches the workflow. Boards often hear from IT, finance, and clinical leadership. They should also hear from unit clerks, billers, pharmacy staff, scheduling teams, and frontline nurses. These are the people who know where the process breaks.
Pilot where pain is obvious
The first pilot should solve a visible problem with a contained workflow. That's not because small goals are safer. It's because trust grows when staff can see the result in their own day.
Good pilot choices usually share three traits:
The workflow is repetitive enough to automate.
The consequences of failure are manageable.
The success criteria are clear to staff, not just executives.
Examples include document intake, referral routing, pre-authorisation support, inventory retrieval workflows, or discharge coordination steps. The pilot should also include a human-centred checkpoint. Ask users whether the tool removed mental effort or merely moved it.
If the pilot saves time for management reports but creates more clicks for nurses, it isn't ready to scale.
Scale through workflow design, not software rollout
Hospitals often “roll out” automation as though deployment is the final milestone. It isn't. Scaling means redesigning the workflow so the tool becomes part of how work is done.
That requires attention to three questions:
| Question | Why it matters |
|---|---|
| Who owns the workflow? | Automation fails when no one owns exceptions and updates |
| What happens when the system is wrong? | Staff need an easy path to override, correct, and learn |
| How will feedback be captured? | Without frontline input, burden creeps back in |
Technical integration also matters here. Data, alerts, and status updates need to move cleanly across systems. Teams planning broader digital coordination may find connected healthcare platforms useful for understanding how interoperability affects adoption.
Build a habit of optimisation
A human-centred roadmap doesn't end at launch. It treats automation as a living workflow.
That means regular review of:
Alert quality: Are notifications helpful or ignored?
Exception handling: Are edge cases creating hidden manual work?
Training needs: Do new staff understand when to trust the system and when to check it?
Emotional load: Do staff say the process feels calmer, clearer, and easier to manage?
The winning implementation mindset is simple. Automate tasks. Protect judgement. Reduce cognitive load wherever possible.
Navigating Canadian Compliance and Security
Compliance often gets framed as the brake pedal on innovation. In healthcare, it should be treated as the steering system. Without it, automation might move quickly but in the wrong direction.
Canadian organisations need to think about privacy, access control, data use, and accountability from the start. That includes obligations under PIPEDA where applicable, plus provincial rules, internal governance standards, and the realities of clinical risk. When automation touches patient data, “we'll secure it later” is not a serious operating plan.
Why compliance improves the business case
Boards sometimes worry that strong governance slows projects. In practice, weak governance slows them more. Teams stall when they don't know which data can be used, who approves access, how audit trails are maintained, or what happens when a model makes an unsafe suggestion.
A compliance-by-design approach asks practical questions early:
Data ownership: Who is responsible for each dataset and workflow output?
Data lineage: Can the organisation trace where information came from and how it changed?
Access controls: Are users limited to the minimum information needed for their role?
Auditability: Can the organisation show what the system did, when, and why?
These controls aren't abstract. They protect patient trust and make procurement, legal review, and operational adoption smoother.
Security should match the workflow, not just the server
Many healthcare teams focus heavily on infrastructure security and not enough on workflow security. Both matter. A secure environment still creates risk if an automated process exposes too much information to the wrong person, or if a generated summary enters a record without proper review.
That's why hospitals need to assess automation at the process level:
| Risk area | Practical control |
|---|---|
| Over-broad access | Role-based permissions and reviewable approvals |
| Unclear outputs | Visible confidence indicators or mandatory review steps |
| Silent failures | Exception queues and escalation paths |
| Poor handling of sensitive data | Strong governance for storage, transfer, and retention |
For leaders reviewing practical steps around safeguarding medical patient data, it helps to compare technical controls with workflow controls. The two are not the same.
Hospitals also need a strong foundation for application and information security across the broader digital estate. This guide to data security in healthcare information systems is useful because it frames security as an architectural concern, not just a policy document.
The strategic point is simple. Compliance is not a tax on automation. It is what makes automation sustainable in Canadian healthcare.
Frequently Asked Questions About Healthcare Automation
Can a small clinic start without a huge budget?
Yes. Start with one narrow workflow that consumes staff time every day. Document intake, appointment follow-up, referral handling, and claims preparation are common entry points because the process boundaries are clear. The first win should be operationally meaningful and easy for staff to judge in daily use.
Avoid a platform-first decision if you haven't defined the workflow problem. A small clinic doesn't need a grand transformation plan. It needs one process that becomes simpler, safer, and less tiring.
Will automation replace staff?
In most healthcare settings, the practical goal is not staff replacement. It's role redesign. Automation handles the repeatable steps so people can focus on exceptions, patient communication, judgement, and coordination.
That said, anxiety is real. Leaders should address it directly. If staff think automation is a hidden workforce reduction programme, adoption drops. If they see it removing frustrating administrative load, adoption improves.
The most successful healthcare automation solutions don't remove the human role. They remove the parts of the role that humans are least well served by doing repeatedly.
What should we ask a vendor before buying?
Ask them to walk through one real workflow from start to finish. Don't accept broad statements about AI, efficiency, or transformation.
Use questions like these:
Where does the data come from, and how is it validated?
What happens when the system can't classify a case confidently?
How are exceptions routed and reviewed?
How do users correct outputs, and does the system learn from that?
What audit trail exists for actions, recommendations, and overrides?
These questions usually reveal whether a product is mature or only packaged well.
How do we evaluate advanced AI, not just basic automation?
Many procurement teams need a sharper framework. A key challenge is ensuring AI agents have “awareness and decision-making capacity” rather than just following rules. Unlike basic automation, these advanced agents require a different implementation and validation strategy to ensure they align with ethical and regulatory guidelines established in Canada, as discussed in Abstracta's analysis of AI-powered systems in Canadian health tech.
In practical terms, that means you shouldn't evaluate an aware AI agent the same way you evaluate a rules engine.
Look for four things:
Decision boundaries
The organisation should know exactly what the agent may decide, suggest, or prioritise.Human oversight
Staff need clear control over review, override, and escalation.Validation in context
Testing should reflect real Canadian workflows, not only generic demo scenarios.Ethical fit
The system should support, not bypass, the governance expectations Canadian healthcare organisations are building around accountability and safety.
An aware AI agent is closer to a junior team member than a checklist macro. That changes how you govern it, test it, and trust it.
Cleffex Digital Ltd helps organisations design and build secure digital systems, including healthcare workflow and AI integration projects, with a focus on practical software delivery. If your hospital, clinic, or healthtech team is assessing how to implement healthcare automation solutions in a way that fits Canadian operational and compliance realities, you can explore Cleffex Digital Ltd for custom development and integration support.







