



McKinsey estimated that up to $250 billion of current US healthcare spend could shift to virtual or virtually enabled care, making telehealth a permanent operating model issue rather than a temporary access channel, as outlined in McKinsey's analysis of telehealth after COVID-19. The strategic question now is no longer whether virtual care will persist. It is how the market will reorganize around it.
That reorganization looks different depending on where an organisation sits in the ecosystem. Providers are redesigning triage, care pathways, staffing, and capacity management. Insurers are reassessing reimbursement policy, fraud controls, network design, and the economics of lower-cost care settings. Software vendors are competing to become part of the clinical and administrative stack, which means supporting interoperability, privacy, documentation, analytics, and patient engagement instead of offering video alone.
This three-sided view matters because telehealth adoption can look healthy for one group while creating pressure for another. A provider may gain capacity but face workflow strain. A payer may reduce avoidable acute utilization but see new overuse patterns in low-acuity care. A vendor may add users quickly but lose relevance if its product sits outside the EHR, claims, and care management workflow.
The next phase of telehealth will be shaped by those interdependencies. Organisations that treat virtual care as an isolated digital feature will struggle to show margin improvement, clinical value, or durable adoption. Organisations that design for the full ecosystem have a better chance of building models that scale. For a practical market view, see AONMeetings telehealth insights.
Beyond the Boom The New Normal for Telehealth
Virtual care use remains well above pre-2020 levels across many health systems. That persistence matters more than the pandemic-era spike because it points to a durable operating change, not a temporary substitution.
Canada is a useful reference point. Virtual care did not snap back to its old baseline after emergency conditions eased. Public funding accelerated adoption early, including a federal investment announced in May 2020, but the more important signal came later. Patients, clinicians, and health system operators kept using virtual channels after in-person care returned. The clearest market signal is not peak demand under constraint. It is steady demand after the constraint disappears.
Stabilisation matters more than surge
Surge reflects urgency. Stabilisation reflects behaviour, workflow redesign, and institutional acceptance.
That distinction changes how each part of the telehealth ecosystem should plan. Providers need to judge virtual care by its effect on triage accuracy, panel capacity, continuity, and follow-up completion. Insurers need to examine whether virtual channels shift utilisation into lower-cost settings or create new low-acuity volume that offsets those savings. Software vendors need to show that their products fit the clinical and administrative stack, especially where scheduling, documentation, billing, and patient communication already live.
A telehealth programme that stays outside those workflows rarely lasts.
Practical rule: If utilisation remains elevated after emergency policy and behaviour normalize, treat telehealth as part of the care model and budget accordingly.
That has direct implications for capital allocation. Health systems should stop treating telehealth as a video line item and start assessing it as infrastructure. The strategic question is whether virtual touchpoints improve throughput, reduce leakage, support chronic care management, and make clinician time more productive. Teams evaluating platform strategy often reach the same conclusion that appears in broader work on connected healthcare platform architecture. Value comes from integration, not from a stand-alone visit tool.
Integration defines the next phase
Three forces now shape telehealth economics and adoption:
Technology maturity that supports monitoring, automation, clinical documentation, and data exchange rather than video alone
Policy and reimbursement changes that determine which services remain payable, under what conditions, and across which jurisdictions
Business model discipline that ties virtual care to measurable clinical and financial outcomes
The same trend creates different incentives across the market. A provider may see telehealth as a capacity-management tool. An insurer may view it as a utilization-management channel with fraud and coding implications. A software vendor may see an opening to become part of the core workflow if it can meet interoperability, privacy, and reporting requirements. Looking at only one of those perspectives leads to poor decisions. A feature that improves access for providers can still weaken payer economics. A product that wins clinician adoption can still fail commercially if it sits outside claims, EHR, and care management processes.
For teams refining operating models, AONMeetings telehealth insights are a useful practical reference because they focus on execution choices rather than abstract digital-health rhetoric.
What separates leaders from laggards
The strongest organisations are no longer asking whether to offer telehealth. They are designing where virtual care belongs in the patient journey and where it does not.
That means making deliberate choices about:
Which encounters should start virtually?
Which pathways should remain hybrid?
Which populations benefit from remote monitoring or asynchronous support?
Which reimbursement and contracting models make those services financially durable?
Telehealth is no longer a side channel. It is part of the delivery model, the payment model, and the software stack. Organisations that plan across all three have a better chance of gaining margin, access, and staying power at the same time.
Understanding the Modern Virtual Care Ecosystem
Most buyers still use “telehealth” as shorthand for a video appointment. That definition is now too small to be useful.
Modern virtual care is a stack of service modalities. Each one suits a different type of clinical interaction, operational goal, and reimbursement reality. The strongest telehealth programmes don't pick one modality. They combine several into a hybrid pathway that matches patient need.
The five parts of the ecosystem
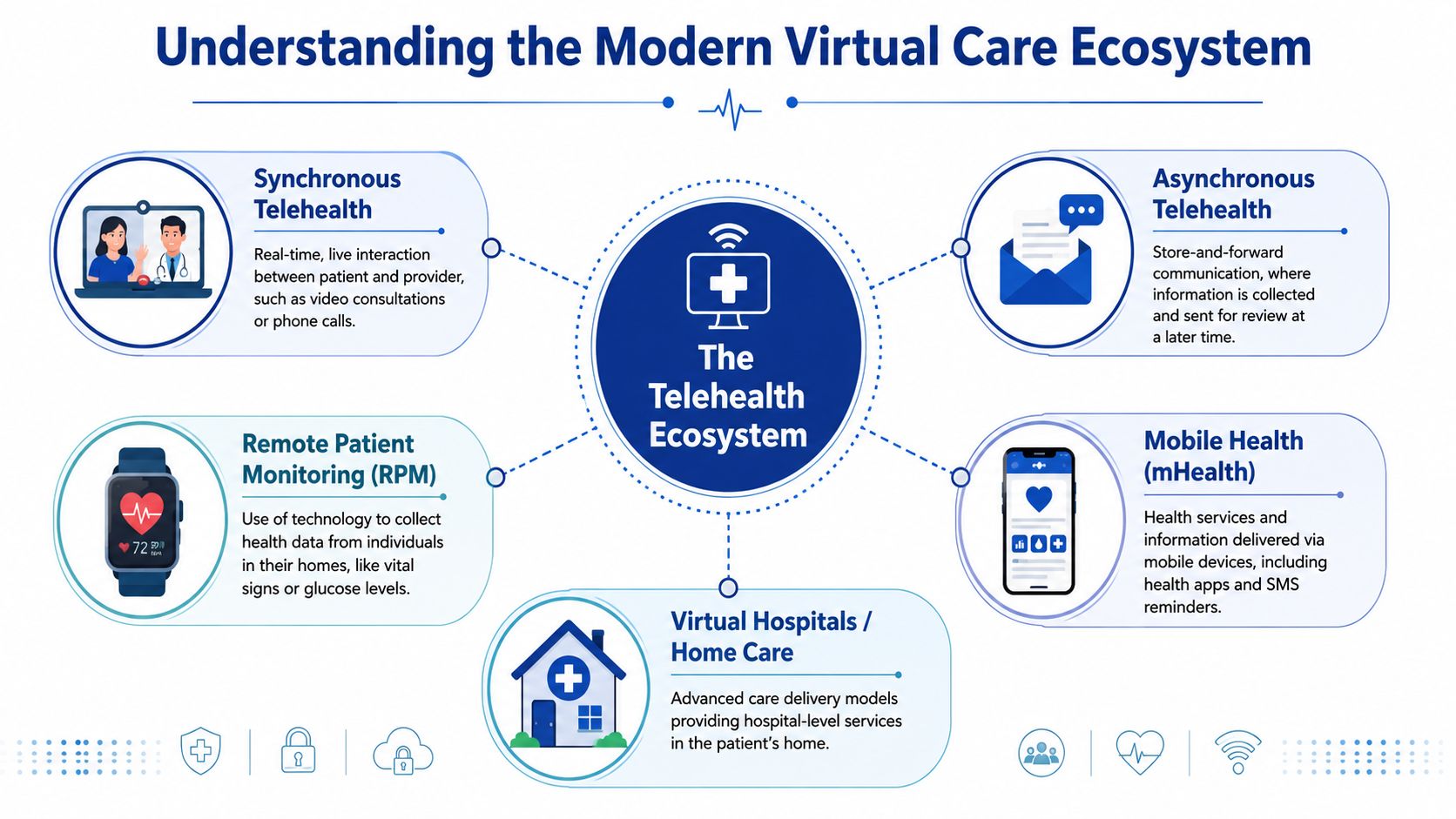
Think of the ecosystem as a communication toolkit rather than a single channel.
Synchronous telehealth works like a live call. Patient and clinician interact in real time through video or audio. It's best when immediate clarification, visual assessment, or rapport matters.
Asynchronous telehealth works more like secure email. Information is collected first, then reviewed later. That suits follow-up questions, image review, refill requests, and administrative touchpoints.
Remote Patient Monitoring adds continuous or recurring clinical data from home devices and wearables. It turns telehealth from episodic interaction into ongoing observation.
Mobile health extends engagement through apps, reminders, symptom prompts, and patient-facing utilities on smartphones.
Virtual hospital and home care models push the concept further by delivering coordinated care in the home that would once have required facility-based support.
Why hybrid care is becoming the default
A single modality rarely handles the full patient journey well. A diabetes pathway, for example, may begin with a live consultation, continue through remote glucose monitoring, and rely on messaging for medication adjustments or education. A post-operative pathway may use one short virtual check-in plus photo-based asynchronous review.
That's why hybrid care keeps outperforming narrow telehealth design in strategic terms. It lets organisations match the channel to the task instead of forcing every interaction into the same format.
Telehealth works best when organisations stop asking which tool is superior and start asking which tool fits the moment in care.
For software vendors, this is a product architecture issue. Platforms built only for live visits often hit a ceiling because care delivery needs tasks, alerts, record exchange, patient messaging, and workflow controls around the visit itself. That's one reason connected infrastructure matters so much. Teams exploring this architecture shift can use this overview of connected healthcare platforms as a practical lens on how those systems fit together.
What each stakeholder should optimise for
The same modality means different things to different buyers.
| Stakeholder | Primary concern | Most relevant modality question |
|---|---|---|
| Providers | Clinical fit and workflow | Which visits can move virtual without lowering care quality? |
| Insurers | Coverage design and utilisation | Which modalities improve access without creating unmanaged fragmentation? |
| Software vendors | Product scope and interoperability | Can one platform coordinate data, communication, and follow-up actions? |
Remote monitoring deserves special attention because it changes the economics and the cadence of care. Buyers looking for a broader market view often review trends in remote patient monitoring to understand where demand is concentrating.
The critical point is that telehealth is no longer a digital front door alone. It's a service mesh. Once leaders see that clearly, technology and policy decisions become much easier to sequence.
Key Technological Drivers Shaping Tomorrow's Telehealth
Telehealth stops being a convenience feature when three technologies mature together. Artificial intelligence, remote monitoring infrastructure, and interoperability each add value on their own. Combined, they create a force multiplier.
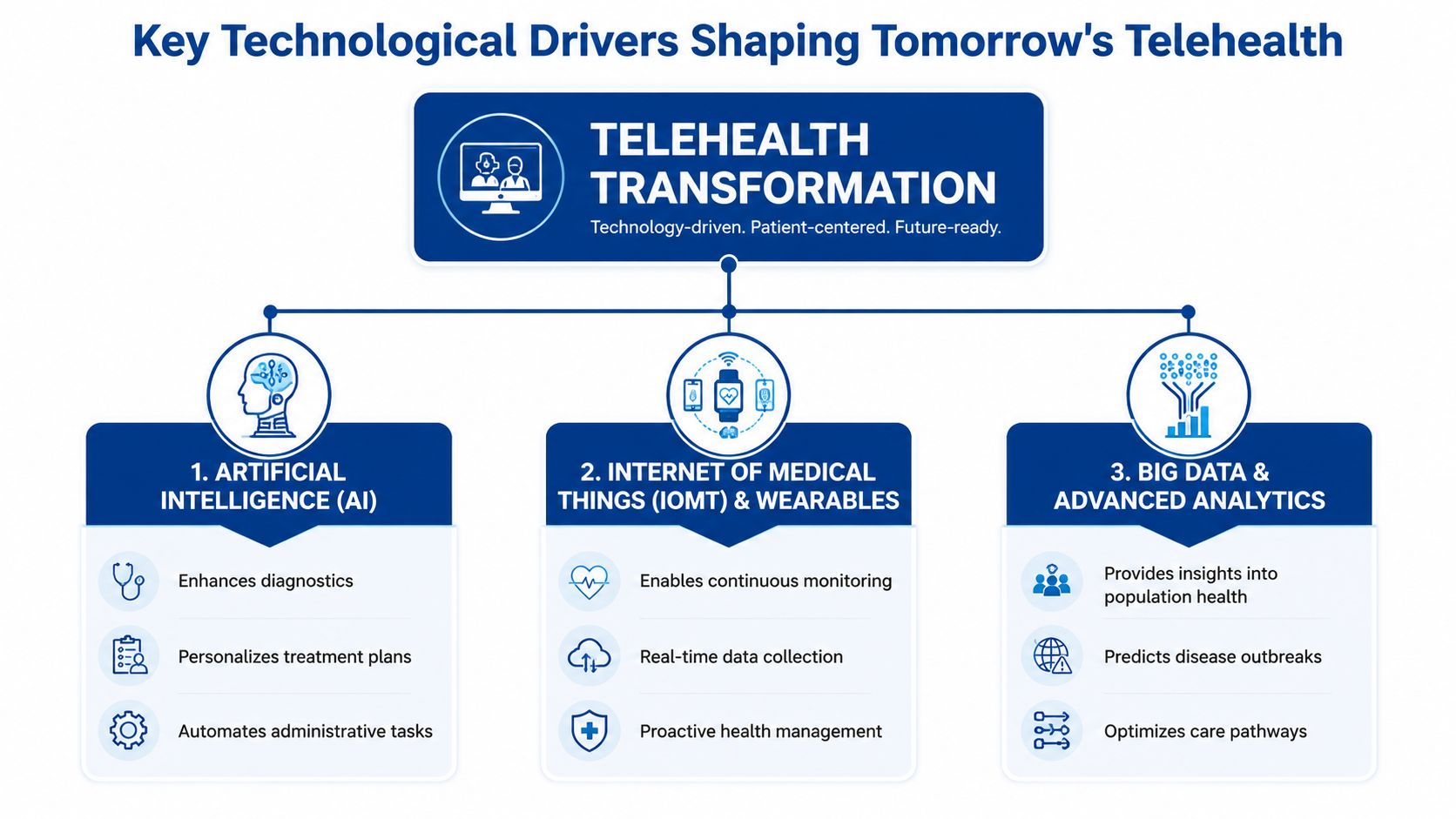
AI is becoming the operating layer
In telehealth, AI matters less as a headline feature and more as invisible infrastructure. The highest-value uses often sit around the clinical encounter rather than replacing it.
AI can support intake classification, route patients to the right service line, summarise clinician notes, flag missing documentation, and help structure follow-up. Those functions matter because telehealth adds operational complexity. A virtual visit still generates consent requirements, scheduling logic, clinical notes, patient instructions, and reimbursement documentation.
For insurers, AI also creates a path to better prior authorisation workflows and more precise routing of members to appropriate care settings. For providers, the gain is administrative relief and cleaner workflow hand-offs. For software vendors, the implication is straightforward. Products that only offer a consultation window will look thin next to platforms that reduce administrative burden around the encounter.
One practical but often overlooked component is speech capture and documentation support. Tools for AI video-to-text conversion are relevant here because telehealth increasingly produces audio and video interactions that need structured summaries, searchable records, and downstream task creation.
RPM changes telehealth from episodic to continuous
The strongest evidence-backed technology trend in the current market is Remote Patient Monitoring. According to Sermo's telemedicine outlook, RPM is emerging as a significant advancement because it enables real-time transmission of vital signs through secure 5G networks. The same source notes that clinical evidence shows RPM reduces wait times and enhances health outcomes for chronic conditions, with strong data supporting its noninferiority to in-person care for diabetes management.
That matters strategically because it changes what telehealth can do. Video solves access to a conversation. RPM solves access to a patient's condition between conversations.
Where RPM creates the most leverage
Chronic care management becomes more proactive because clinicians can review trends instead of waiting for deterioration to become obvious.
Specialty access improves in areas where travel, appointment scarcity, or rural coverage makes continuous follow-up difficult.
Insurer programme design becomes more refined because interventions can be tied to actual patient status rather than fixed check-in intervals.
Providers should also note that RPM requires a different service design than ordinary teleconsultation. Someone has to review incoming data, define escalation thresholds, and connect alerts to clinical action. Vendors that ignore that operational layer tend to sell devices without delivering a workable care model.
Interoperability is the hard prerequisite
The future of telehealth depends on whether virtual encounters become part of the patient record or remain trapped in separate systems.
When data from visits, messages, monitoring devices, and in-person care can't move cleanly across systems, telehealth creates fragmentation rather than continuity. Clinicians lose context. Claims teams lose clarity. Patients repeat themselves. The cost isn't just inconvenience. It's lower trust in the digital channel.
The winning platform isn't the one with the most features. It's the one that fits into the clinical and administrative workflow with the least friction.
That's why APIs, standards-based exchange, identity management, and integration with EHR environments are now core product requirements. Teams evaluating build-versus-buy choices can frame these requirements through a telemedicine software development guide that maps architecture decisions to healthcare-specific constraints.
The combined effect
AI improves the efficiency of decisions and documentation. RPM extends observation beyond the appointment. Interoperability turns those signals into coordinated care rather than isolated digital events.
That combination is where the market is heading. Not towards telehealth as a video service, but towards telehealth as an intelligent clinical workflow.
Navigating the Evolving Regulatory and Reimbursement Maze
Policy now determines which telehealth models scale, which stall, and which never reach profitability. For providers, insurers, and software vendors, the regulatory question is no longer whether virtual care is permitted. It is whether a specific service line can be delivered compliantly, paid for consistently, and defended under the same clinical scrutiny as in-person care.
California offers a clear reference point. The Medical Board of California's telehealth guidance states that telehealth is a mode of delivering care, not a separate standard of practice. Physicians treating patients located in California must hold a valid California licence and meet the same standard of care expected in person.
That distinction matters because many organisations still treat telehealth policy as a procurement or compliance checklist. It is closer to operating strategy. Clinical appropriateness, licensure, consent, documentation, prescribing rules, and privacy controls all shape what can be offered, to whom, and at what margin.
The standard of care stays constant
Virtual care does not reduce the clinician's duty to choose the right modality, document the encounter properly, or escalate to in-person care when the case requires examination, testing, or intervention. The legal and clinical exposure remains with the treating organisation.
The implications differ by stakeholder.
Providers need governance that defines which visit types are suitable for phone, video, asynchronous messaging, or remote monitoring, and when handoff to physical sites is required. Insurers need coverage rules that separate legitimate substitution from avoidable utilization. Software vendors need product design and sales claims that align with regulated workflows, rather than suggesting that software can bypass them.
A telehealth platform that increases visit volume without improving clinical triage can create downstream cost and liability for all three groups.
Reimbursement determines whether access expands or contracts
Payment policy is often the hidden force behind telehealth adoption curves. Temporary parity rules can stimulate rapid uptake. Narrow billing criteria, lower rates, or platform-specific requirements can just as quickly compress supply.
Ontario illustrates the point. Under the province's current physician payment framework, virtual billing depends on specific code rules, eligibility criteria, and technology conditions set by the Ontario Health Insurance Plan and the Ministry of Health, including distinctions between video and telephone services and requirements tied to insured primary care relationships, as outlined in the Ontario Schedule of Benefits for Physician Services and ministry virtual care guidance. The strategic lesson is broader than one province. Reimbursement design does not just influence claims processing. It affects clinician behaviour, patient access, and the economics of platform investment.
That creates different strategic pressures across the ecosystem. Providers must decide whether telehealth supports retention, panel management, and follow-up efficiency under actual fee schedules, not headline demand. Insurers must judge where virtual care lowers total cost of care versus where it adds a second billable touchpoint. Vendors must build products flexible enough to support multiple reimbursement models, because a workflow optimised for parity-based fee-for-service may fail in capitated, employer-sponsored, or value-based arrangements.
Three questions every organisation should ask
Licensing reach
Can clinicians legally treat patients across the geographies the organisation plans to serve, including cross-state or cross-provincial edge cases?Privacy alignment
Does the service model fit the applicable health privacy and consumer data rules, including storage, consent, recording, and third-party data flows?Payment durability
Are current reimbursement rules stable enough to justify investment in staffing, workflow redesign, and product integration, or are they still transitional?
The strongest telehealth strategies treat regulation and reimbursement as product inputs, not external constraints. That is the difference between a virtual care offering that remains a pilot and one that becomes a durable line of business.
Breakthrough Use Cases and Profitable Business Models
The most valuable telehealth use cases are no longer confined to routine primary care. The field is broadening into service lines where digital delivery solves a specific operational bottleneck, access gap, or follow-up problem.
Behavioural health is a strong example because continuity and privacy often matter more than physical examination. Chronic disease programmes fit well when clinicians need repeated touchpoints, education, and tracking over time. Post-operative follow-up can benefit when the main question is whether recovery is progressing as expected and whether symptoms justify escalation. Virtual physical therapy can work when guided exercises, coaching, and periodic reassessment are more important than facility-based equipment.
What makes a use case commercially sound
A telehealth use case becomes durable when it has three traits:
Clear clinical boundaries so teams know what can remain virtual and when to escalate
Operational repeatability so scheduling, documentation, and follow-up don't become bespoke every time
A payment path through direct consumer spend, payer partnerships, employer contracts, or provider budgets
That's why many telehealth ventures fail when they market broad convenience instead of solving one expensive or frustrating problem well. Buyers don't want a generic platform. They want lower friction in a known workflow.
A profitable telehealth model usually starts with a narrow care journey and expands from there, not the other way round.
Comparison of Telehealth Business Models
| Model | Target Customer | Revenue Stream | Key Success Factor |
|---|---|---|---|
| Direct-to-consumer subscription | Patients | Recurring subscription or visit fee | Strong brand trust and a simple user journey |
| Provider SaaS platform | Hospitals, clinics, speciality groups | Software licence, implementation, support | Workflow fit inside clinical operations |
| Insurer partnership model | Health plans and payer-led programmes | Contracted service delivery or care-management arrangement | Demonstrable effect on access and care coordination |
| White-label telehealth infrastructure | Digital health brands and enterprise healthcare operators | Platform licensing and custom development | Configurability, compliance, and integration depth |
| Speciality virtual care network | Referral groups, employers, patients | Episode-based fees, contract revenue, or blended models | Clinical focus in one service line |
Matching use cases to models
A behavioural health platform may perform well with a direct-to-consumer model if access and continuity are the main value proposition. A chronic care solution with monitoring often fits better through provider or insurer contracts because it depends on longitudinal care coordination. A post-operative pathway may be best delivered as part of a hospital or speciality group's existing service offer rather than as a standalone product.
Software vendors should pay close attention to this alignment. The same underlying capabilities can support multiple business models, but packaging, compliance responsibilities, onboarding, and reporting requirements will differ.
Where margin and defensibility come from
The biggest margin driver isn't usually the consultation itself. It's the surrounding workflow.
Vendors and operators create defensibility when they own pieces such as triage logic, structured intake, device integration, claims-ready documentation, multilingual communication, or care-plan orchestration. Providers gain an advantage when telehealth reduces bottlenecks in scarce specialities or follow-up pathways. Insurers create value when virtual channels improve access without creating disconnected care episodes.
The future of telehealth will reward business models that connect clinical usefulness to operational discipline. Convenience brought people in. Service design will determine who stays profitable.
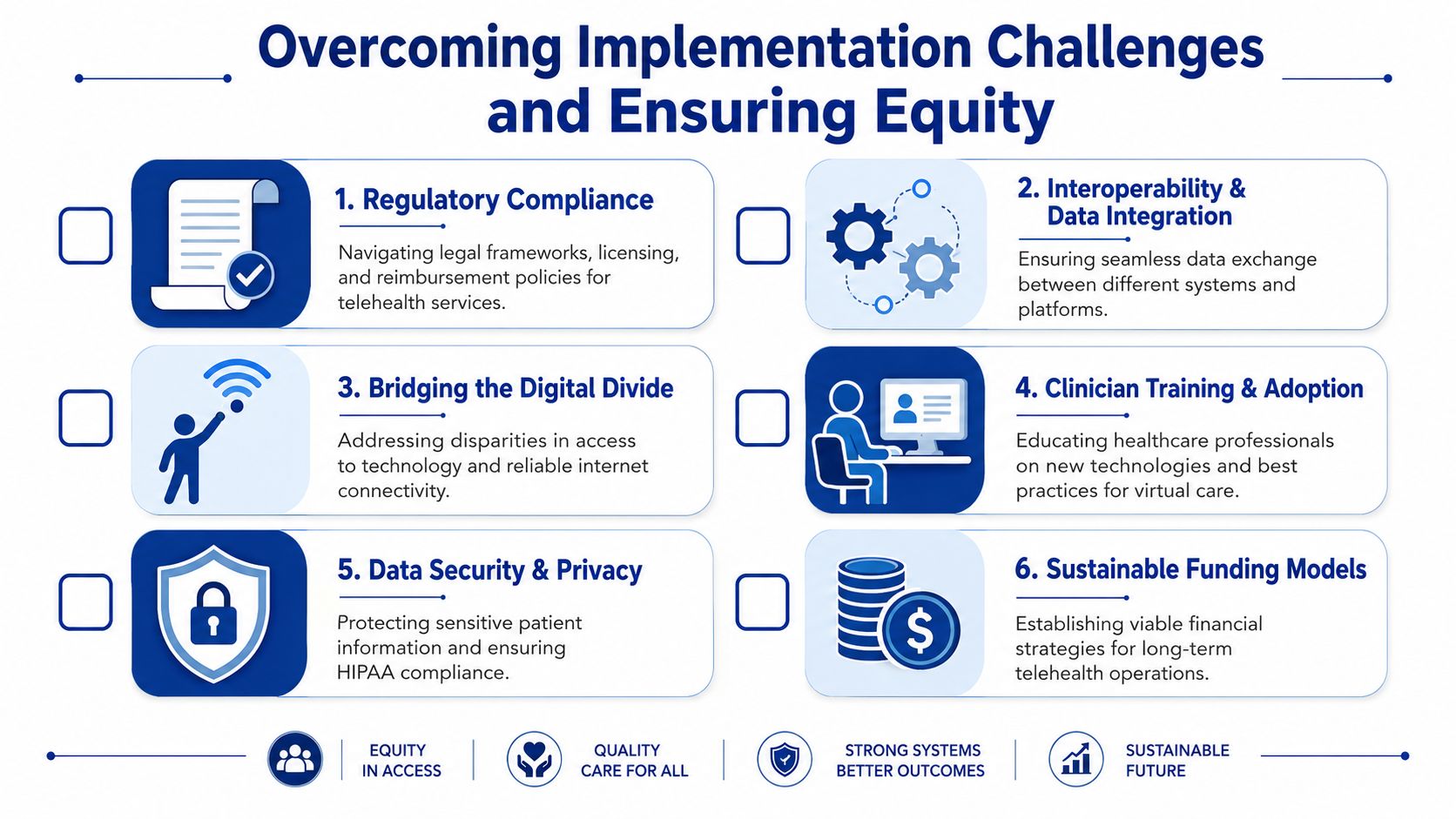
Overcoming Implementation Challenges and Ensuring Equity
Most telehealth rollouts don't fail because the video works poorly. They fail because the organisation underestimates workflow change, governance effort, and patient access barriers.
That's why implementation should be treated as a change-management programme with technical dependencies, not as a software deployment with a few training sessions attached.
Equity has to be designed in
The sharpest warning sign comes from language access. In California, telehealth usage among non-English speaking and limited English proficiency populations was 4.8% compared with 12.3% for English-proficient patients, even though 22% of residents had limited English proficiency, according to the Health Affairs analysis on telehealth disparities. That gap shouldn't be treated as a side issue. It tells leaders that digital access is not the same as equitable access.
If language support, culturally adapted interfaces, and community-level digital literacy aren't built into the service, telehealth can widen the very access gaps it claims to solve.
The practical barriers leaders overlook
Workflow fit: Clinicians need rules for modality selection, escalation, and task ownership after the visit.
Data integration: Telehealth data has to land where care teams can use it.
Training: Staff need operational playbooks, not just platform logins.
Security: Privacy controls have to cover the full interaction, including messaging, storage, and device-linked data.
Funding logic: Leaders need a durable view of who pays for what and under which policy conditions.
What better implementation looks like
An equitable telehealth programme usually includes a mix of design and operating choices.
Language-aware interfaces: Patient instructions, consent flows, and reminders should reflect the language reality of the population served.
Assisted onboarding: Some patients need support before the first appointment, especially if they're unfamiliar with patient portals or mobile apps.
Hybrid fallback routes: When video isn't workable, organisations need alternate paths that preserve continuity rather than recording a failed encounter.
Clinician scripts and protocols: Providers should know how to identify when digital communication is becoming unsafe, unclear, or insufficient.
Operational insight: Equity work becomes scalable only when it's embedded in product design, intake workflow, and staff incentives at the same time.
Why this is a business issue, not only a public-interest issue
Providers that ignore equity leave clinical demand unmet. Insurers that ignore it create access distortions in member populations. Vendors that ignore it build products that look polished in demos but underperform in real deployment.
The future of telehealth belongs to organisations that design for variation in language, literacy, connectivity, and care complexity from the beginning. Accessibility isn't a feature layer. It's part of whether the service works at all.
Seizing the Opportunity in a Digital-First Healthcare Future
The commercial case for telehealth now rests on persistence, not novelty. In Canada, 56% of telemedicine users in 2023 intended to continue using virtual care post-pandemic, and 74% wanted to maintain or increase their usage frequency, according to Capterra's analysis of telemedicine demand in Canada. That's the clearest signal a strategist needs. Patient behaviour has shifted enough to support long-term investment.
Where providers should move next
Providers should stop framing telehealth as an access add-on and start treating it as a service-line design tool. The most promising paths are pathways where virtual triage, follow-up, education, and monitoring can reduce friction without weakening clinical judgement.
That means building around targeted care journeys, not launching generic digital clinics. It also means selecting platforms that support documentation, messaging, and escalation rules rather than only appointment delivery.
Where insurers can create leverage
Insurers have a larger role than paying claims for virtual visits. They can shape the future of telehealth by encouraging hybrid models that improve continuity, by aligning reimbursement with clinically appropriate use, and by supporting programmes that connect members to care before conditions worsen.
The strongest insurer strategies will likely combine network design, data-sharing expectations, and member experience standards. Telehealth works best when it closes care gaps, not when it creates another disconnected point solution.
Where software vendors have the clearest opening
For software companies, the opportunity is not “another telemedicine app”. The opening is in solving the hard parts:
Compliance-aware workflow tools for regulated clinical environments
RPM platforms that connect device data to actionable care processes
Middleware and integration layers that reduce fragmentation between EHRs, claims systems, and patient-facing tools
AI-supported operations for intake, summarisation, and follow-up coordination
Language-sensitive interfaces that serve populations often excluded from digital care
That broader strategic shift is part of a wider healthcare technology transition that this perspective on digital transformation and healthcare captures well.
The real market signal
The future of telehealth won't be won by whoever offers the most virtual visits. It will be won by the organisations that make virtual care clinically credible, operationally efficient, and accessible to more people without increasing fragmentation.
That's the 360-degree view the market often misses. Providers need care-model discipline. Insurers need payment and access logic. Software vendors need infrastructure thinking. When those three line up, telehealth stops being a standalone category and becomes part of the core healthcare system.
Cleffex Digital Ltd helps organisations turn that shift into working software. If you're building secure telehealth platforms, connected care systems, AI-enabled healthcare workflows, or compliant patient engagement tools, Cleffex Digital Ltd can support custom development with an agile approach shaped for complex healthcare environments.







