



It's 8:15 on a Monday morning. The waiting room is already full, phones are ringing, your triage nurse is juggling incomplete intake notes, and one patient who looked stable at the door suddenly needs faster attention than anyone first realised.
That's the setting where AI-powered patient triage systems stop sounding like a technology trend and start looking like an operational necessity. For a hospital innovation committee, the appeal is straightforward. You want safer prioritisation, smoother intake, and fewer avoidable delays without making clinicians feel that software is second-guessing their judgement.
In Canadian care settings, that conversation has to be more practical than promotional. The actual question isn't whether AI can sort symptoms on a screen. It's whether your organisation can deploy it in a way that fits local workflows, protects privacy, handles bias responsibly, and earns enough clinician trust to be used in real life.
Beyond the Clipboard: The New Front Door to Care
A paper clipboard used to be the symbolic front door to care. Today, the front door is broader. It includes online intake, symptom capture, voice interfaces, digital check-in, and the logic that decides who should be seen first.

An AI-powered patient triage system is best understood as an intelligent support layer at intake. It gathers information from what the patient says, what the chart already contains, and what staff record at arrival. Then it helps rank urgency, suggest routing, and flag cases that deserve a second look sooner rather than later.
That matters because triage isn't only about clinical safety. It's also about flow. A bottleneck at intake spreads everywhere else: exam rooms, urgent consults, handoffs, scheduling, and discharge planning. Hospitals that are already investing in digital access tools are increasingly treating triage as part of the same strategic problem as portals, self-service forms, and messaging. That's why teams often connect this work to a broader digital patient engagement strategy, rather than treating it as a stand-alone purchase.
Why the market is moving quickly
Adoption is accelerating well beyond pilot-stage curiosity. The AI-Powered Patient Triaging market was valued at $2.8 billion in 2025 and is projected to reach $12.4 billion by 2033, growing at an 18.6% CAGR according to a systematic review on AI-powered patient triaging. For innovation leaders, that doesn't prove any one product works. It does signal that providers, vendors, and investors all see triage as a core workflow worth redesigning.
Practical rule: Don't frame AI triage as “automation replacing intake staff.” Frame it as better risk sorting at the earliest possible moment.
What this looks like on the ground
In practice, the technology may sit in several places:
Before arrival: Patients enter symptoms through a web form, app, chatbot, or phone-based system.
At reception: Front-desk staff or nurses use guided prompts instead of relying only on free-text notes.
During triage: The system highlights urgency cues that might otherwise be buried in incomplete or rushed documentation.
After intake: Routing options can include self-care advice, virtual review, urgent clinic assessment, or emergency escalation.
The attraction is simple. If the front door works better, the rest of the building usually does too.
How AI Patient Triage Systems Work
Most non-technical leaders don't need model architecture diagrams. They need a usable mental model. The simplest one is this: think of AI triage as a digital medical detective.
It listens to the patient's story, checks for clues in the chart, notices patterns in vitals, and then offers a recommendation about urgency. It doesn't replace the clinician who makes the final call. It helps that clinician notice risk sooner and organise intake more consistently.
The two core engines
Two technical pieces matter most.
First is Natural Language Processing, or NLP. This is the part that interprets unstructured language. If a patient says, “I feel pressure in my chest and it started while walking upstairs,” NLP helps the system interpret the meaning of that complaint instead of treating it as random text. In the emergency triage context, the referenced NEJM AI analysis described AI tools using NLP to interpret unstructured chief complaints.
Second is supervised machine learning. This is the pattern-recognition engine trained on historical examples. It looks at structured inputs such as vital signs and other recorded data, then estimates the likelihood of outcomes that matter for triage.
From input to action
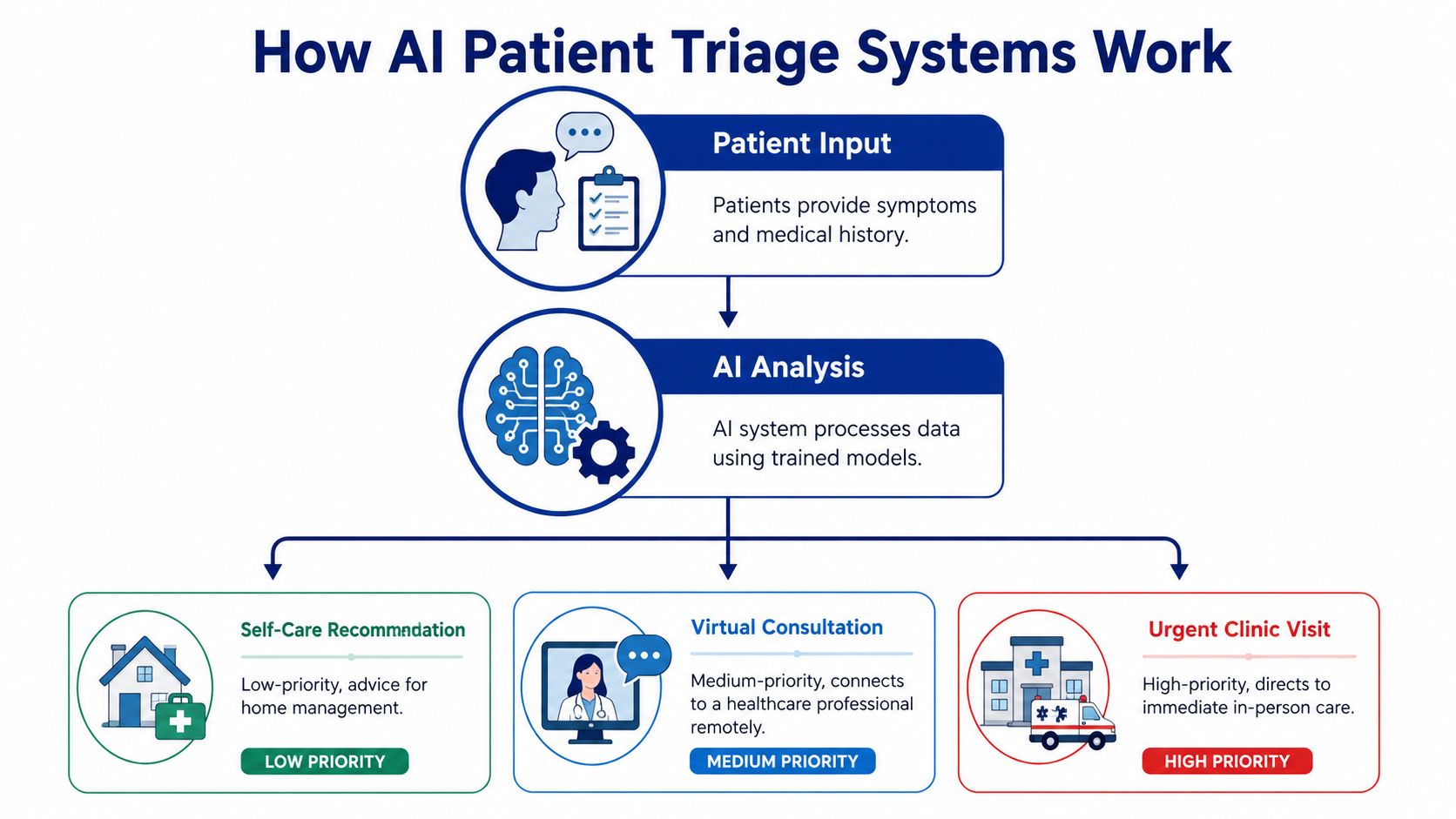
A useful way to explain the flow to clinicians and administrators is to break it into a short sequence:
Patient information is captured: That may include symptoms, history, observations, and vital signs.
The AI analyses the information: NLP handles the words. Machine learning handles the measurable inputs and outcome prediction.
A triage recommendation is generated: The system might suggest lower-acuity guidance, virtual assessment, urgent in-person review, or immediate escalation.
A clinician reviews and acts: In a well-designed deployment, the recommendation supports judgement rather than bypassing it.
Leaders who want to compare this with other clinical support tools usually find it helpful to read a broader primer on AI clinical decision support, because triage is one subset of that larger category.
Good AI triage systems don't “know medicine” the way a nurse or physician does. They recognise patterns, structure messy intake data, and make those patterns easier for clinicians to use.
Where people often get confused
The biggest misunderstanding is thinking triage AI is the same thing as diagnosis. It isn't. Triage asks, “How urgent is this, and where should this patient go next?” Diagnosis asks, “What condition does this patient have?” Those are related, but they aren't the same task.
Another common confusion is assuming all AI triage tools work only through patient-facing chatbots. Some do. Others sit inside intake software, call-centre workflows, or emergency department triage screens. The interface changes, but the core purpose stays the same: sort urgency earlier and more reliably.
The Clinical and Operational Impact
Committees usually approve this kind of project for two reasons. The first is patient safety. The second is operational performance. AI-powered patient triage systems matter only if they improve one or both.
The strongest evidence in the material you provided comes from a landmark NEJM AI study summarised in an Iatrox review of AI-powered triage in emergency departments. Across 174,648 emergency department visits across three sites, the AI-informed triage tool improved identification of critical care patients from 78.8% to 83.1%. The same implementation was associated with a 33% reduction in median time from patient arrival to the initial care area, from 12 minutes to 8 minutes.
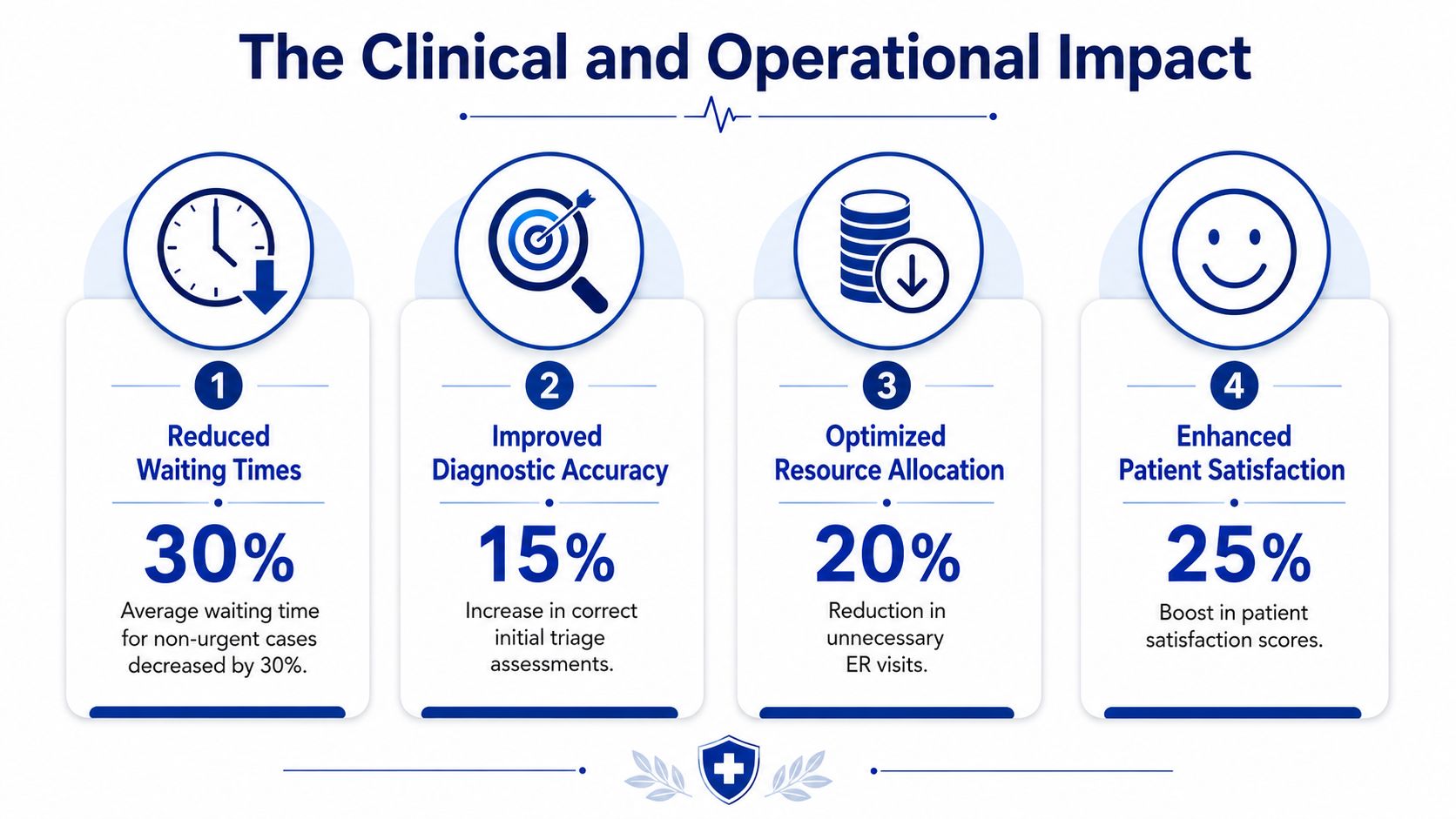
That's the kind of result that gets executive attention because it links triage logic to both acuity recognition and throughput.
What those gains mean operationally
A few practical implications follow from those findings.
Earlier recognition of high-risk patients: When critical cases are identified more reliably, teams can accelerate placement, monitoring, and escalation.
Faster movement out of intake: Shorter time to the initial care area can reduce congestion where risk is hardest to manage.
Better use of staff attention: Clinicians spend less energy re-sorting patients whose acuity was underestimated at the front door.
The same review also noted that machine learning models outperformed conventional triage scoring systems such as the Emergency Severity Index for predictive accuracy related to hospital admission, ICU admission, and mortality. For committees, the key takeaway isn't that old methods are obsolete. It's that AI can add a stronger prediction layer than rule-based scoring alone.
The less visible operational benefit
There's another gain that often matters more after go-live than before. Documentation gets easier when the intake process is structured well.
The systematic review cited earlier found that Voice-AI systems achieved a 19% faster documentation speed compared with manual methods in clinical triage settings. It also reported that machine learning algorithms reduced mis-triage rates within a documented range, and that screened studies showed statistically significant improvements in diagnostic accuracy and efficiency over clinician-assigned ESI scores, especially in critical situations. That supports a practical point many leaders already suspect: administrative friction and clinical risk are often tangled together.
If your triage workflow still depends on rushed transcription, inconsistent wording, and scattered intake screens, accuracy problems and flow problems usually show up at the same time.
What to watch when interpreting the evidence
A committee should still ask hard questions.
One emergency department study doesn't guarantee the same effect in a community clinic. A voice-first model may help one site and frustrate another. A strong prediction score in testing may fail if the local workflow forces staff to ignore the recommendation.
So the right conclusion isn't “AI triage works everywhere.” The right conclusion is narrower and more useful. When the model, workflow, and staff adoption align, measurable improvements are possible.
Your Implementation Roadmap From Pilot to Practice
Most AI triage failures aren't caused by bad intentions. They're caused by treating implementation like a software install instead of a service redesign.
A practical roadmap starts with operational questions, not procurement questions: where is delay happening now, which staff role is overloaded., which decisions are inconsistent, and which patient groups are being routed too late, too early, or with too much manual rework?
Phase one and two
Start with a focused scope.
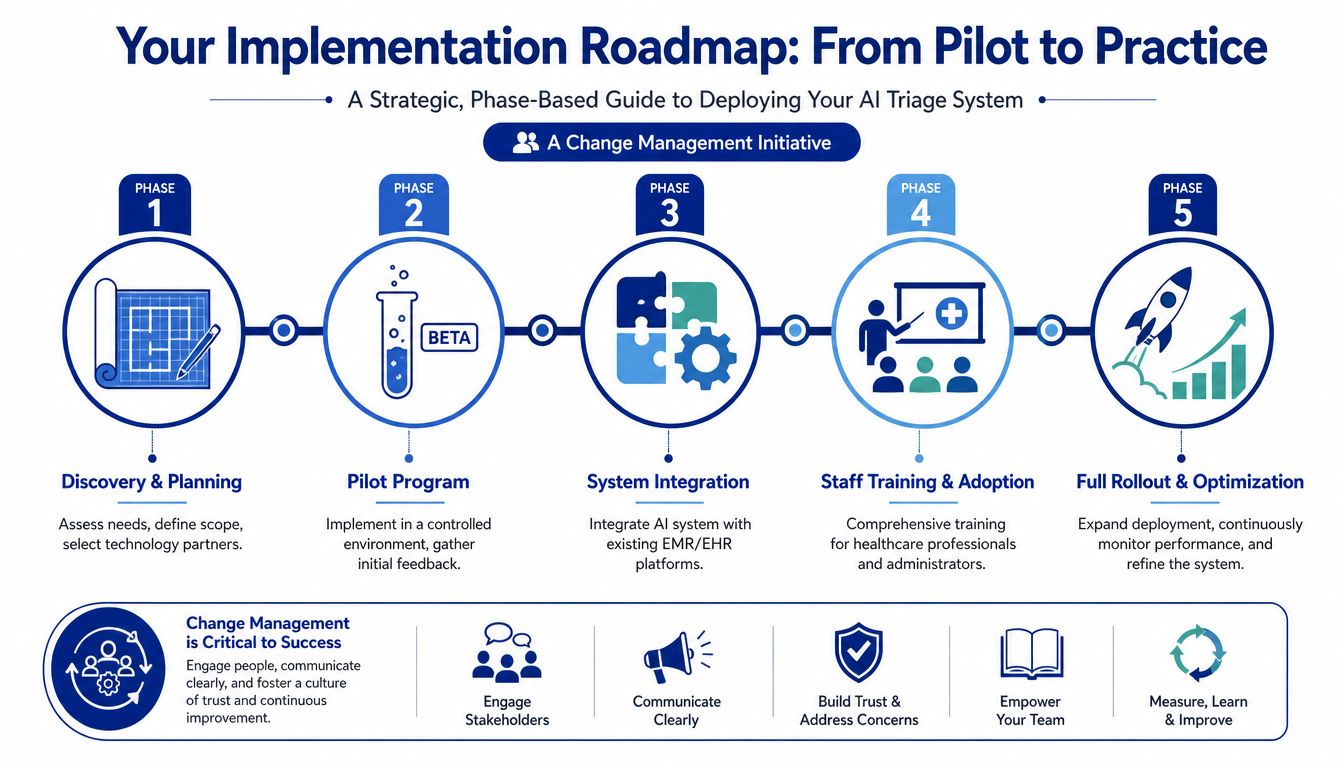
Discovery and planning
Pick one triage setting first. That might be emergency intake, after-hours nurse routing, a same-day clinic queue, or a digital symptom intake flow. Define success in operational terms your managers already use, such as faster prioritisation, cleaner documentation, or fewer handoff corrections.Pilot programme
A pilot should be controlled enough to learn from but realistic enough to expose workflow friction. Include clinical leaders, frontline triage staff, privacy officers, IT, and operations from the beginning. If one of those groups is missing, the pilot usually produces a partial answer to the wrong question.
Phase three and four
Technical fit matters, but so does training.
System integration: Connect the triage tool to your EMR or EHR, identity management, and intake workflows. If staff have to swivel between too many screens, they'll stop trusting the process even if the model itself performs well.
Staff training and adoption: Clinicians don't just need logins. They need examples of when to follow the recommendation, when to override it, and how those overrides will be reviewed. Many organisations now build short scenario-based modules and convert slide decks into reusable video assets. A guide on optimising presentations for video learning can help teams turn implementation training into something staff will revisit.
Phase five
Scaling should happen only after local validation.
A sensible rollout checklist looks like this:
Review override patterns: Are clinicians disagreeing with the system for good reasons, or because the interface is awkward?
Audit edge cases: Look closely at paediatrics, language barriers, mental health presentations, and patients with complex histories.
Refine workflow ownership: Decide who investigates triage discrepancies, who updates pathways, and who signs off on operational changes.
Expand gradually: Move to new sites or services in stages rather than all at once.
A pilot isn't successful because it proves the vendor's demo worked. It's successful because it reveals what your clinicians need before the system goes wider.
One practical note on tool selection during implementation: some organisations use patient-facing triage chat interfaces as part of the intake layer. For example, Cleffex Digital Ltd offers healthcare AI chatbot solutions that can support symptom triage and patient routing as one possible component within a broader workflow design. That kind of tool still needs the same governance, integration, and local validation as any other triage product.
Navigating Compliance Privacy and Validation
Canadian deployments face significant challenges. An AI triage tool can look impressive in a vendor walkthrough and still create unacceptable risk if its training data, accountability model, or privacy posture don't fit your environment.
The most uncomfortable issue is also the most important one: bias. In Canada, a major concern is whether commercial models have been validated on data that adequately reflects Indigenous communities, recent immigrants, and other underrepresented populations. A source focused on Canadian health innovation notes that while AI triage can reduce wait times by 50% at some Canadian hospitals, there is a critical validation gap around sufficient Indigenous or recent immigrant health data, with associated risk of misdiagnosis, and clinician trust remains a major barrier because there are no clear legal liability protocols when AI triage gets it wrong, as described in this Canadian healthcare innovation discussion.
What Canadian leaders should ask before go-live
Use these questions in governance review, not just procurement:
Whose data trained the model?
Ask whether the vendor can describe representativeness in a Canadian context.
How is local validation done?
You need evidence from your own patient population and workflow, not only general product claims.
Can clinicians understand the recommendation?
Explainability matters because staff won't rely on a black-box suggestion when stakes are high.
Who is accountable for errors?
You need a written escalation and liability framework before frontline use.
Privacy and legal fit
Canadian privacy compliance isn't a box-ticking exercise. If the system handles personal health information, leaders need to examine data residency, access controls, retention, auditability, and vendor contract language under the rules that apply to their province and operating model. A practical starting point is this overview of AI in healthcare data privacy in Canada.
Hospitals that don't yet have an internal AI oversight structure may also benefit from an external framework for policies, review boards, and risk assignment. For that, this primer on F1Group AI governance support is a useful reference for shaping a governance model before procurement moves too far.
The governance question isn't whether the AI can recommend a triage level. It's whether your organisation can explain, defend, monitor, and correct that recommendation in practice.
Validation should be ongoing
Don't treat validation as a one-time pre-launch event. Models interact with changing patient mix, staffing patterns, documentation habits, and policy changes. A system that appears acceptable at launch can drift operationally if nobody reviews outcomes, clinician overrides, or subgroup performance after rollout.
For Canadian committees, that's the heart of responsible adoption. The technology may be new. The duty of care isn't.
Choosing the Right AI Triage Partner
Vendor selection gets messy when buyers compare feature lists instead of implementation reality. The safer approach is to assess partners across clinical, technical, governance, and service criteria at the same time.
Budget also needs to be grounded early. The cost of integrating AI into a triage system can range between $40,000 and $400,000 or more, reflecting the work required for scalable, secure, and compliant deployment, as reported in the earlier systematic review. That range should change the tone of the conversation. You're not buying a plug-in. You're funding a clinical workflow capability.
What to evaluate first
A good partner should be able to answer questions such as:
Technical fit: Will it integrate cleanly with your current systems and identity controls?
Clinical validation: Can the vendor show evidence of safe performance in settings that resemble yours?
Security and compliance: Where is data stored, who can access it, and how are audits handled?
Implementation support: Who trains staff, supports pilots, and helps revise workflows after deployment?
Here's a practical screening table your committee can use.
AI Triage Vendor Evaluation Checklist
| Evaluation Category | Key Questions to Ask | Look For |
|---|---|---|
| Technical fit | How does the system connect to our EMR, intake tools, and communication channels? | Clear integration approach, workable user experience, minimal duplicate data entry |
| Clinical validation | What evidence do you have for the care settings we operate? How are recommendations reviewed by clinicians? | Transparent validation approach, local pilot readiness, clear override process |
| Compliance and security | Where does health data reside? How are permissions, logs, and retention managed? | Canadian privacy awareness, audit trails, role-based access, contract clarity |
| Partnership model | What happens after go-live? Who handles training, workflow tuning, and incident review? | Named implementation support, realistic rollout plan, governance collaboration |
Red flags worth noticing
Some warning signs appear before legal review ever starts.
A vendor may talk confidently about “accuracy” but avoid discussing subgroup performance. Another may promise smooth clinician adoption without showing a training plan. Some products generate polished triage outputs but don't fit the way nurses document or hand off patients. Those gaps are expensive.
The best partner for your organisation won't necessarily be the one with the flashiest interface. It'll be the one that can show how its product behaves inside your constraints.
The Future of Patient-Centred Triage
AI-powered patient triage systems are reshaping the first clinical decision in the care journey. That makes them strategically important. It also makes them sensitive, because mistakes at intake echo through everything that follows.
For Canadian providers, the opportunity is real. Better prioritisation, cleaner intake, and more consistent routing can improve both patient care and day-to-day operations. But the strongest programmes won't be the ones that install AI fastest. They'll be the ones that validate locally, train carefully, monitor bias, and define accountability before trouble appears.
The most useful way to think about AI triage is as augmented judgement. The software can structure information, surface risk, and support consistency. Clinicians still provide context, empathy, and final responsibility.
That balance matters. Patients don't experience triage as a model, a dashboard, or a procurement category. They experience it as the moment someone decides how urgently they need help, where they should go, and whether they feel seen. If AI improves that moment without weakening trust, it earns its place.
If your organisation is exploring secure, compliant digital health workflows, Cleffex Digital Ltd can help you evaluate and build the software layers around modern triage, from patient-facing intake experiences to healthcare AI integrations designed for real operational use.







