



Canadian healthcare teams are under pressure to offer digital access that patients will use, while still meeting privacy, security, and operational requirements. For clinics, hospitals, and insurers, digital patient engagement now affects intake, reminders, education, claims communication, billing, and follow-up. The question is no longer whether digital channels belong in the care journey. The harder question is which channels improve outcomes, reduce staff friction, and justify the investment.
In practice, that requires more than adding a portal or turning on automated texts. A useful strategy has to fit the realities of Canadian care delivery: provincial privacy obligations, uneven access to devices and broadband, bilingual or multilingual communication needs, and patient populations with very different levels of digital confidence. Teams that ignore those constraints usually end up with low adoption, fragmented workflows, and weak ROI.
I see the same pattern across organisations. Engagement efforts often start as a technology purchase and stall because no one has defined success in operational terms. Lower no-show rates, faster intake completion, fewer avoidable calls, better medication adherence, higher portal activation in the right patient groups, and more timely claims or care-plan communication are better starting points.
Digital engagement also sits inside a broader digital transformation strategy for healthcare organisations. The difference is execution. Patients judge the experience one task at a time, booking an appointment, reading prep instructions, submitting a form, asking a question, or understanding what happens next. If those steps are secure, clear, and easy to complete, organisations see measurable gains. If they are confusing or exclusionary, digital tools add cost without improving care.
Why Digital Patient Engagement Is No Longer Optional
Patients already expect to handle basic healthcare tasks digitally. Appointment reminders, intake forms, follow-up instructions, bill notices, and simple service questions now compete with the standards patients see in banking, retail, and public services. Clinics and insurers that still depend on phone queues, paper packets, and manual follow-up create avoidable friction before care even starts.
That shift has operational consequences. If a patient cannot confirm an appointment after hours, complete forms before arrival, or get a clear next step without calling the office, staff absorb the work. Schedules run less efficiently. Call volumes rise. Missed steps show up later as no-shows, delayed intake, unpaid balances, repeat outreach, and lower patient confidence.
Digital engagement is now part of service delivery.
The mistake I still see is treating it as an add-on channel instead of a workflow decision. A portal alone does not fix fragmented communication. Automated texts do not help much if replies go nowhere. A telehealth visit does not remove front-end friction if consent, triage, identity checks, and follow-up still happen through disconnected processes. Real improvement comes from linking patient-facing touchpoints to the work teams already do in scheduling, registration, care management, and billing.
What Changes in Day-to-Day Operations
In practical terms, digital patient engagement affects three areas first:
Access: Patients can book, confirm, reschedule, or complete pre-visit tasks without waiting for office hours.
Workload: Front-desk and contact-centre teams spend less time on repetitive reminders, form chasing, and status calls.
Continuity: Patients receive guidance between visits, which reduces dropped handoffs and unclear next steps.
The trade-off is real. Digital channels reduce manual effort only when they are set up with ownership, escalation rules, and clear service standards. Otherwise, organisations add one more inbox, one more queue, and one more place where patients get stuck.
This is also why patient engagement cannot sit outside a broader digital transformation strategy for healthcare organisations. Internal systems matter, but patients judge the organisation by whether they can complete simple tasks securely and without confusion. If that experience breaks, the investment in back-office technology is harder to justify.
Why Delay Is Expensive
Postponing digital engagement usually creates costs that do not show up cleanly on a budget line:
Administrative drag: Staff handles repeatable tasks that patients could complete themselves.
Communication gaps: Reminders, prep instructions, benefit updates, and care-plan messages are sent inconsistently across channels.
Equity risk: Patients with limited digital confidence, language barriers, or inconsistent device access are left with a poor fallback experience instead of an inclusive one.
Weak ROI: Organisations buy tools but cannot connect them to measurable outcomes such as lower no-show rates, faster intake completion, or fewer avoidable calls.
That last point gets ignored too often. Digital patient engagement is not worth doing because it sounds modern. It is worth doing when the model is practical, secure, inclusive, and measurable. For providers, that means fewer avoidable operational failures. For payers, it means clearer member communication and lower service friction. For patients, it means less effort to get through the system.
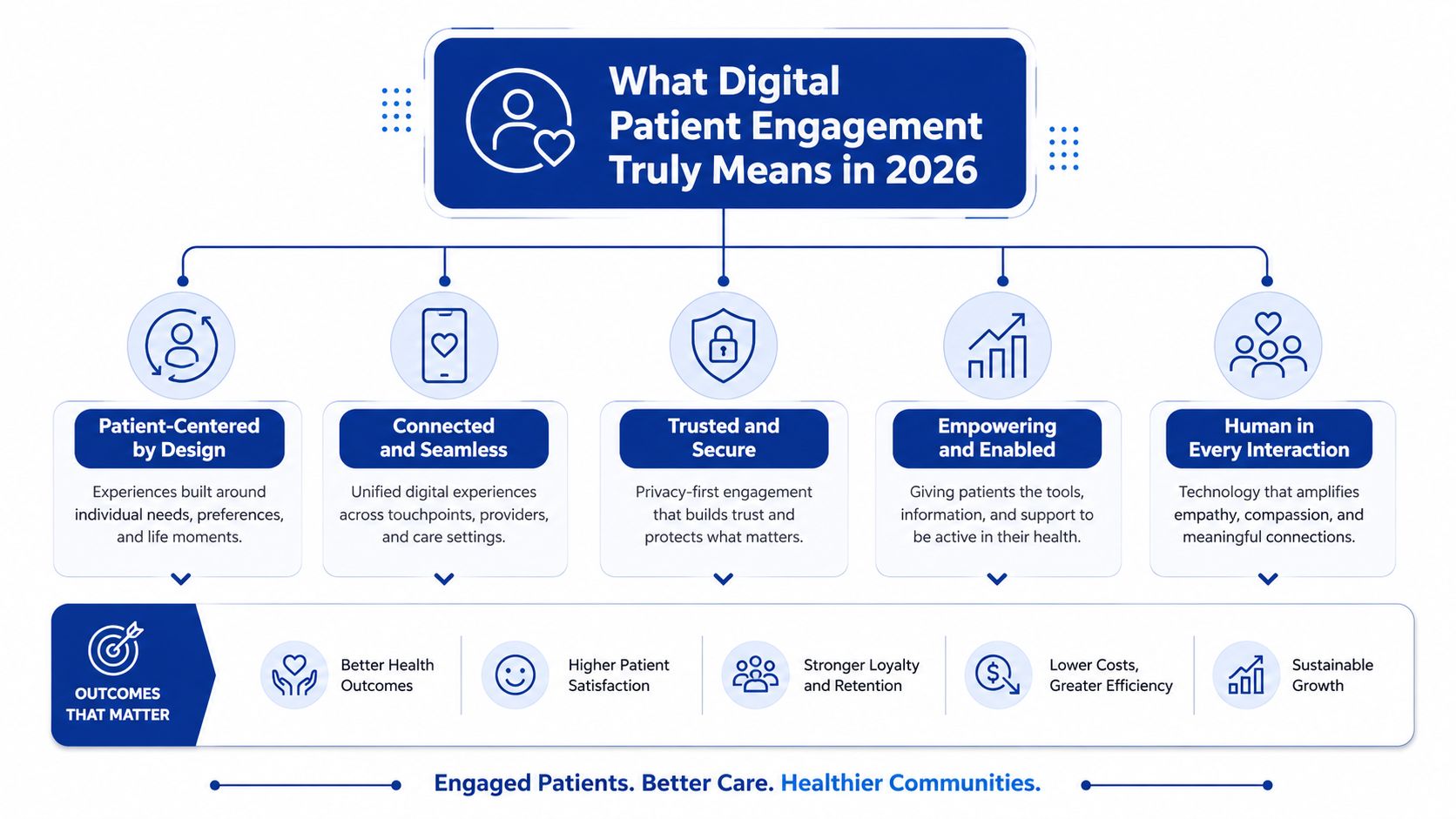
What Digital Patient Engagement Truly Means in 2026
Many teams still define digital patient engagement too narrowly. They think of reminders, portal logins, or the occasional telehealth visit. That misses the operational scope of the work.
Leading research presents a more useful model. Digital engagement spans three operational dimensions: access to care, financial activity, and healthcare information, with examples such as online booking, confirmations, online bill payment, digital check-in, and test result viewing. The same research notes that digital bill payment and electronic statements showed the highest growth from 2021 to 2024, according to Athenahealth's patient digital engagement research.
Here's the simplest way to think about it. Digital patient engagement is the digital front door and the digital service desk working together.
The Three Pillars That Matter
Access to Care
This is the front-end experience. Patients need simple ways to book, confirm, reschedule, or cancel. If these tasks still depend on business hours or long hold times, friction builds early.
This pillar often determines whether patients complete the first step at all.
Financial Activity
Many organisations underestimate the importance of the billing experience. Patients don't separate clinical care from administrative friction. If payment options are awkward, statements are unclear, or online billing is clumsy, the experience breaks down after the visit.
Financial workflows are part of engagement because they shape completion, trust, and staff workload.
Healthcare Information
Patients need access to forms, check-in steps, results, instructions, and follow-up information in formats they can use. However, many digital programmes fall short in this regard. They publish information, but don't make it timely, understandable, or actionable.
What This Means for Strategy
A mature engagement model doesn't ask, “Do we have a portal?” It asks:
Can patients complete the next task easily?
Can staff see where patients get stuck?
Do communication and transactions happen in one connected flow?
Working rule: If a patient still needs to call for basic administrative tasks, your digital front door is only half built.
This broader definition matters because it turns engagement into something measurable. It also helps clinical and operational teams work from the same framework, rather than treating digital tools as separate projects.
Key Benefits for Providers, Payers, and Patients
The value of digital patient engagement looks different depending on who is using it. Providers want less friction and fewer manual tasks. Payers want better member communication and better support for care plan follow-through. Patients want convenience, clarity, and less confusion.
But there's an important caveat. Many public-facing articles promise benefits without meaningful evaluation, and the more important question for Canadian organisations is which interventions effectively help reduce missed appointments or improve adherence. That gap is highlighted in this review of digital health engagement evidence.
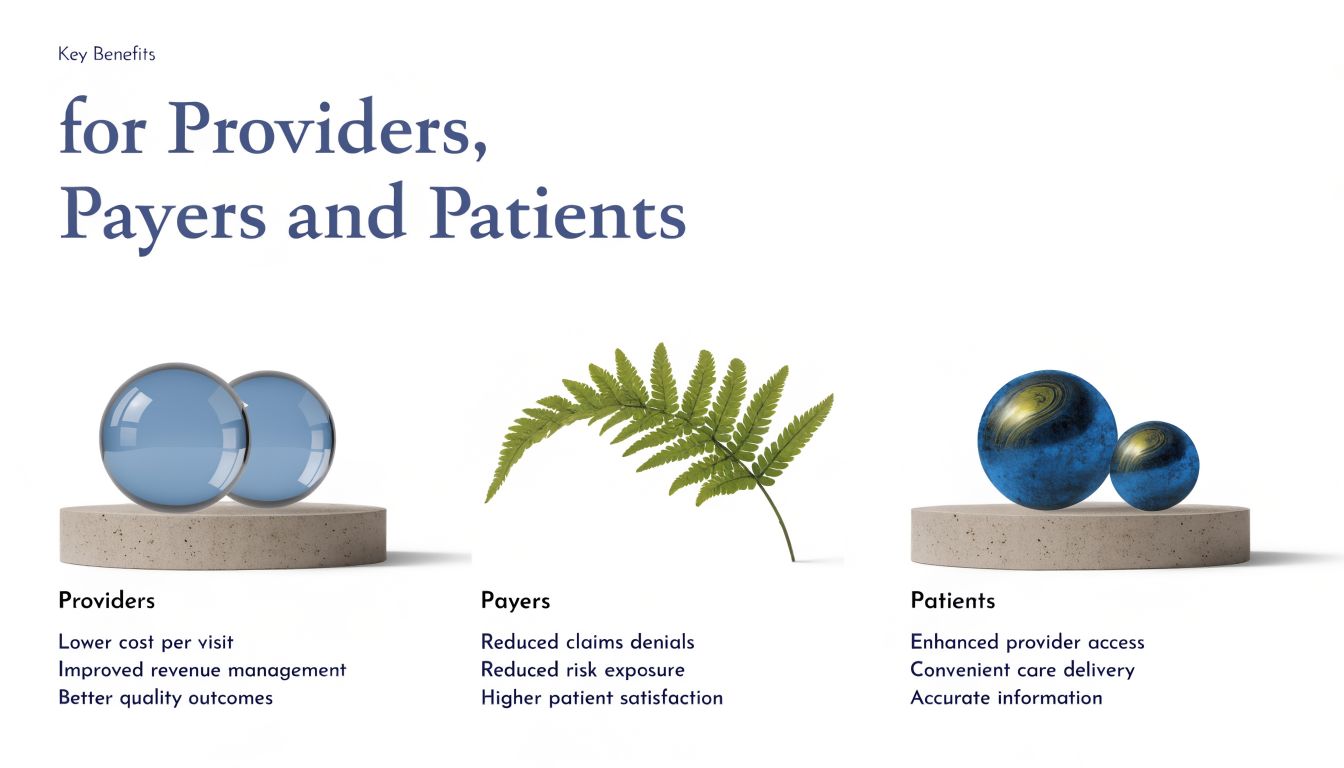
For Providers
Providers usually feel the impact first in operations.
Lower administrative burden: Self-service booking, reminders, and digital intake reduce repetitive front-desk work.
Stronger revenue processes: When billing and statements are easier to access, payment workflows become less manual.
Better workflow visibility: Teams can see whether tasks were completed instead of guessing based on call volume.
The trap is assuming these results appear automatically. They don't. If the platform is hard to use, if messages are poorly timed, or if staff don't know how to intervene when patients drop off, the system creates new work.
For Payers
Payers benefit when communication becomes more timely and structured. Digital engagement can support plan education, preventative outreach, reminders, and navigation support across a broader member journey.
What matters most is coordination. If outreach is generic, too frequent, or disconnected from member needs, people ignore it. If it's tied to clear actions and support pathways, it becomes more useful.
For Patients
Patients usually judge engagement by one standard. Did it make healthcare easier to manage?
Useful digital engagement can help patients:
Understand next steps
Access information without chasing staff
Handle routine tasks at convenient times
Stay connected between visits
The patient doesn't care whether a task sits with scheduling, billing, clinical ops, or IT. They care whether they can get it done.
What Separates Real ROI From Wishful Thinking
If an organisation wants to show value, it should measure behaviour and completion, not just tool adoption. Good questions include:
Which reminders lead to confirmed appointments
Which messages trigger follow-up tasks
Where patients abandon forms or booking
Which groups engage less and need different support
That's how digital patient engagement becomes a business case rather than a buzzword.
Exploring the Technology Behind Patient Engagement
Most healthcare teams don't need more tools. They need fewer disconnected ones. The technology stack for digital patient engagement should support the patient journey with the least possible friction.
That's why channel choice matters so much. Best-practice guidance from Health Catalyst stresses simplifying communication channels, noting that many patients won't install an app or manage portal passwords, while SMS remains a low-friction channel on devices patients already carry.
Channel Choice Is a Design Decision
A common mistake is pushing every interaction into the portal. Portals are useful, but they aren't ideal for every task. If a patient has to remember login details just to confirm an appointment, response rates often suffer. If the task is sensitive, detailed, or document-heavy, the portal may still be the right place.
The point isn't to choose one channel. It's to match the channel to the task.
| Channel | Primary Strength | Best Use Case |
|---|---|---|
| SMS | Low friction and fast response | Reminders, confirmations, simple prompts |
| Patient portal | Secure access to records and tasks | Results, secure messaging, forms, statements |
| More room for context | Education, follow-up summaries, billing notices | |
| Mobile app | Richer ongoing experience | Frequent users, chronic care pathways, loyalty-style engagement |
| Telehealth platform | Direct remote consultation | Virtual visits, follow-up reviews, care access |
| AI chatbot | Immediate navigation support | FAQs, triage routing, scheduling hand-off |
What Tends To Work Best
SMS for Simple Actions
If the goal is confirmation, preparation, or a quick nudge, SMS often works well because it doesn't require setup. It meets patients where they already are.
Portals for Secure Transactions
Portals still matter. They're appropriate for results, records, secure messaging, and payment-related functions. They just shouldn't be the only doorway.
Telehealth for Specific Care Moments
Telehealth is valuable when the clinical interaction itself can happen remotely. It isn't a substitute for broader engagement workflows around intake, education, reminders, and follow-up.
Where AI and Workflow Tools Fit
AI can support patient engagement when it narrows effort instead of adding noise. A chatbot can route common questions, help patients reach the right service, or support appointment handling. Speech and documentation tools can also reduce friction for staff and improve the speed of follow-up communication. Teams evaluating workflow efficiency may also find this guide to medical speech-to-text technology helpful, especially where clinician documentation delays affect patient-facing updates.
One practical example from the market is Cleffex's patient engagement technology perspective, which aligns software choices with healthcare workflows rather than treating engagement as a standalone feature.
A good engagement stack doesn't ask patients to learn your systems. It adapts to the way patients already communicate.
What Doesn’t Work Well
App-first strategies for occasional users
Portal-only communication for time-sensitive tasks
Too many alerts without a clear priority
Tools that don't connect to scheduling, CRM, or EHR workflows
Technology decisions should start with one question. What is the patient trying to do, and what is the simplest, secure way to help them do it?
How To Ensure No Patient Is Left Behind
Digital access and digital inclusion aren't the same thing. A system can launch a portal, automate reminders, and still leave large parts of its population behind.
That happens because portal use is often uneven. Research on digital health equity notes that access is frequently concentrated among more privileged groups, with barriers linked to digital literacy, language, and device access. It also argues that true equity requires both digital and non-digital options, plus patient involvement in design, as discussed in this review on patient portal equity and implementation.
Inclusion Has To Be Operational
Equity can't sit in a slide deck. It has to show up in daily workflow decisions.
A few examples make the point:
A senior patient may prefer a phone call for complex instructions but still welcome SMS reminders.
A newcomer may need multilingual onboarding before they can use digital forms confidently.
A rural patient may have intermittent connectivity, making lightweight channels more practical than app-based workflows.
If the programme assumes every patient is digitally confident, it will skew towards the easiest-to-serve users.
Practical Ways To Reduce Exclusion
Keep Non-Digital Routes Open
Digital-first shouldn't mean digital-only. Patients should still be able to call, ask for help in person, or receive printed instructions when needed.
Co-Design With Real Patient Groups
Bring patients and families into testing early. Don't rely only on internal assumptions about what's intuitive.
Support Onboarding Directly
Some patients need one-to-one help with first login, form completion, or understanding where to find information. That support is often the difference between adoption and abandonment.
Monitor by Patient Group
Engagement dashboards should show more than aggregate usage. Teams need to look for patterns by age, language, geography, and other relevant factors so gaps become visible.
Equity test: if your highest-need patients are the least likely to use the tool, the design needs work.
The Trade-Off Organisations Must Accept
Inclusive engagement is less tidy than a portal-only model. It involves multiple channels, extra support, and more careful measurement. But that complexity reflects the actual world.
The strongest programmes don't force every patient down the same route. They create a flexible path that still protects privacy, supports staff, and gives patients a realistic way to participate.
Your Step-by-Step Implementation Roadmap
Digital patient engagement projects usually break down into two places. Teams buy a platform before they define the service model, or they launch a pilot and cannot prove whether it reduced calls, improved completion, or changed staff workload. Both problems are avoidable.
A workable roadmap starts with one operational question. Which patient interaction creates enough friction, volume, and cost that fixing it will produce a measurable return?
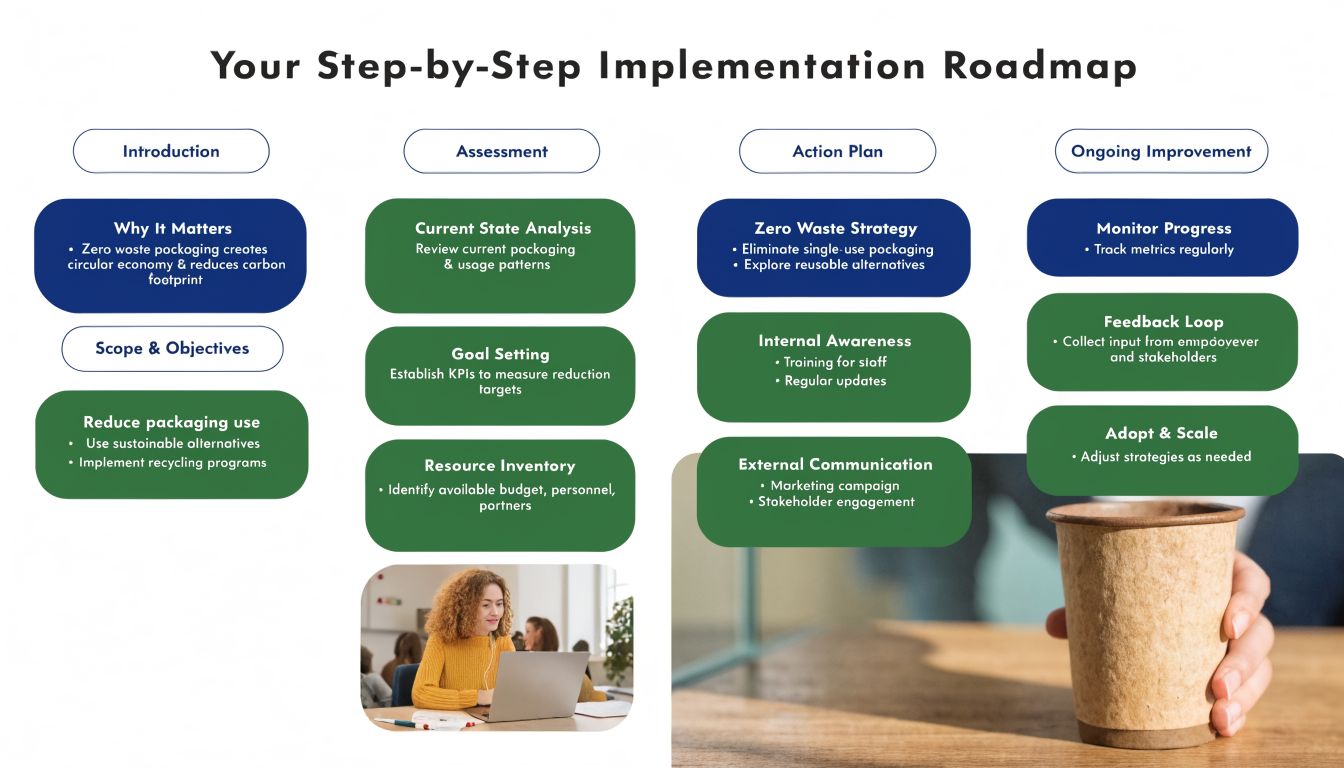
Editor's note: Replace this image with a healthcare or software implementation roadmap graphic. The current image is unrelated to patient engagement and will confuse readers.
Phase One: Define the Use Case and Business Case
Start small enough to control, but important enough to matter. Good starting points include appointment confirmation for a speciality clinic, digital intake for a high-volume service line, or post-discharge follow-up for members with a known readmission risk.
The first job is not software selection. It is a process definition.
Map the current workflow from the patient's point of view and the staff's point of view. Identify where work stalls, where manual follow-up starts, and where errors create downstream cost. Then set success measures tied to operations and finance, such as fewer no-shows, higher form completion before arrival, faster payment collection, or fewer calls to the front desk.
This planning stage often overlaps with patient relationship management and workflow orchestration. A useful reference is Cleffex's perspective on CRM software for the healthcare industry, especially for organisations trying to connect communication history, outreach rules, and service workflows.
Phase Two: Choose Technology That Fits the Workflow
A platform should support the journey you designed. It should not force staff into a new maze of clicks just because the vendor demo looked polished.
For providers, the shortlist usually comes down to a few practical checks:
Integration fit: Connection to scheduling, EHR, billing, CRM, and call centre tools
Security and consent controls: Role-based access, message audit trails, consent capture, and clear data handling rules
Channel support: SMS, email, portal messaging, and outbound call workflows where needed
Operational reporting: Dashboards that show completion, exceptions, delays, and staff intervention
Configuration effort: What your team can realistically maintain after go-live
There is a trade-off here. More features can create more complexity, longer implementation, and a greater training burden. In many clinics, a narrower stack that solves one journey well produces better results than an enterprise tool deployed too broadly.
Phase Three: Pilot in a Live Setting
Run the first rollout in a real environment with a defined patient population, a named owner, and a limited set of rules. Broad launches hide failure. Pilots expose it early enough to fix.
A practical pilot plan includes:
One high-friction workflow
Clear inclusion and exclusion criteria
Staff training on normal flow and exception handling
Plain-language patient instructions
A short review cycle during the first weeks of use
For example, a multisite clinic might pilot digital intake only for follow-up visits in one department before extending it to new patients, where forms are longer, and identity verification is stricter. An insurer might start with renewal reminders for one member segment before applying the model to broader outreach. Both approaches reduce risk and make ROI easier to measure.
Phase Four: Measure Outcomes That Matter
Delivery rates are not enough. Sent messages do not equal completed actions.
Measure what happened after the outreach. Did patients confirm, check in, submit forms, pay, schedule, or call for help? Did staff workload fall, shift, or rise because exceptions increased? Did one patient group complete the journey at a lower rate than others?
The metrics should answer four questions:
Was the message received?
Was the task completed?
Where did human intervention occur?
Did the workflow save time or revenue compared with the old process?
This is the point where many programmes lose discipline. If leadership asks whether the investment worked, teams need more than usage screenshots. They need evidence tied to operations, cost, and patient follow-through.
Phase Five: Standardise What Works and Retire What Does Not
After the pilot, decide what earns expansion. Keep the workflows that improve completion, lower avoidable manual work, and hold up under real staffing conditions. Rework or retire the ones that look good in reports but create confusion at the front line.
Standardisation matters because ad hoc digital engagement creates governance problems fast. Message templates drift. Consent handling becomes inconsistent. Reporting definitions change by department. A shared operating model prevents that.
The organisations that do this well treat digital patient engagement as a service line capability, not a one-time deployment. They assign ownership, review performance regularly, and budget for iteration. That is how theory turns into a secure, measurable programme that leadership can defend as a business case.
The Future of Patient Engagement Is Collaborative
The strongest digital patient engagement strategies don't rely on technology alone. They combine workflow design, patient-centred communication, operational discipline, and inclusion.
That's the part many organisations miss. A portal launch isn't a strategy. An SMS tool isn't a strategy. Even an AI assistant isn't a strategy. Those are components. The essential work is deciding how patients move through access, information, communication, and payment in ways that are simple, secure, and measurable.
Collaboration matters because no single team owns the full experience. Operations owns the flow. Clinical teams' own relevance. IT owns integration and security. Patient access teams own usability. Leadership owns the business case. Patients themselves should shape the design, especially where equity gaps are likely.
For healthcare organisations that want to modernise, the practical target is clear. Reduce friction. Measure completion. Keep alternatives open for people who need them. Build trust by making each interaction easier than the last.
Teams looking for support with healthcare software, secure patient-facing workflows, and digital product delivery can explore Cleffex healthcare services.
If your organisation is rethinking how patients book, communicate, access information, and stay engaged across the care journey, Cleffex Digital Ltd can help you design and build secure, workflow-led healthcare solutions that are practical to implement and easier to measure.







