



A hospital administrator sees the same pattern every week. Patients move through triage, consults, diagnostics, discharge planning, and follow-up, yet the process still feels improvised. One team updates the EMR. Another sends manual reminders. A third tracks gaps on spreadsheets because the system doesn’t show the full journey in one place.
A startup founder in digital health faces a similar problem from the other side. The product works, clinicians are interested, and the care model makes sense. But once real patients enter the flow, operational friction appears everywhere. Messages are missed, handoffs slow down, and no one agrees on which metric proves the service is working.
That’s where HealthcareOps becomes useful. It gives healthcare teams a practical way to connect people, workflows, systems, and feedback so care delivery becomes more reliable, easier to improve, and easier to scale.
The Growing Need for Operational Excellence in Healthcare
A typical morning in a Canadian clinic can unravel quickly. A receptionist is chasing missing referral notes. A nurse is trying to confirm whether lab work was completed. A physician is documenting in the EMR while also checking whether a patient received a follow-up call. None of these tasks is unusual. The problem is that they often happen in separate systems, with separate owners, and without a shared operational view.

That friction isn’t just annoying. It affects access, continuity, and staff capacity. The pressure is even sharper in underserved areas. Over 4.5 million Canadians lack access to a family physician. In rural provinces, Health Professional Shortage Area rates are 25% higher than in urban centres, according to this analysis of underserved populations in healthcare. When access is already limited, broken workflows make a hard problem worse.
Why the Old Operating Model Struggles
Most organisations didn’t design their processes for today’s mix of in-person care, virtual care, patient messaging, remote monitoring, and compliance demands. They added tools over time. The result is patchwork operations.
Common signs include:
Manual coordination everywhere: Staff move information between inboxes, portals, spreadsheets, and the EMR.
Invisible bottlenecks: Teams know delays exist, but they can’t see exactly where patients stall.
Unclear ownership: Clinical, operational, and technical teams solve problems separately instead of together.
Documentation drag: Administrative burden eats into time that should go to patients.
One useful way to ease that documentation burden is to look at tools that reduce note-taking friction. For teams assessing that part of the workflow, this 2026 guide for medical speech-to-text offers a practical overview of how voice-driven documentation fits into clinical operations.
Practical rule: If staff need a workaround to deliver routine care, the workflow needs to be redesigned, not just more effort.
Why CareOps Matters Now
HealthcareOps is a response to this operational reality. It treats care delivery as something that can be designed, monitored, and improved continuously. That matters for a small clinic trying to reduce missed follow-ups, and it matters for a larger health system trying to align virtual care, discharge planning, and patient communications under one operating model.
In plain terms, CareOps helps healthcare teams stop relying on heroic effort. It replaces ad hoc coordination with organised care flows that can hold up under pressure.
What Is HealthcareOps?
HealthcareOps is the discipline of designing, running, and improving healthcare delivery as an operational system. If DevOps helped software teams ship changes faster and more reliably, CareOps applies a similar mindset to care pathways, patient journeys, and service operations.
The central idea is simple. Care isn’t only clinical. It’s also logistical, administrative, digital, and financial. When those parts don’t work together, patient experience suffers, and staff lose time. CareOps creates a shared method for coordinating them.
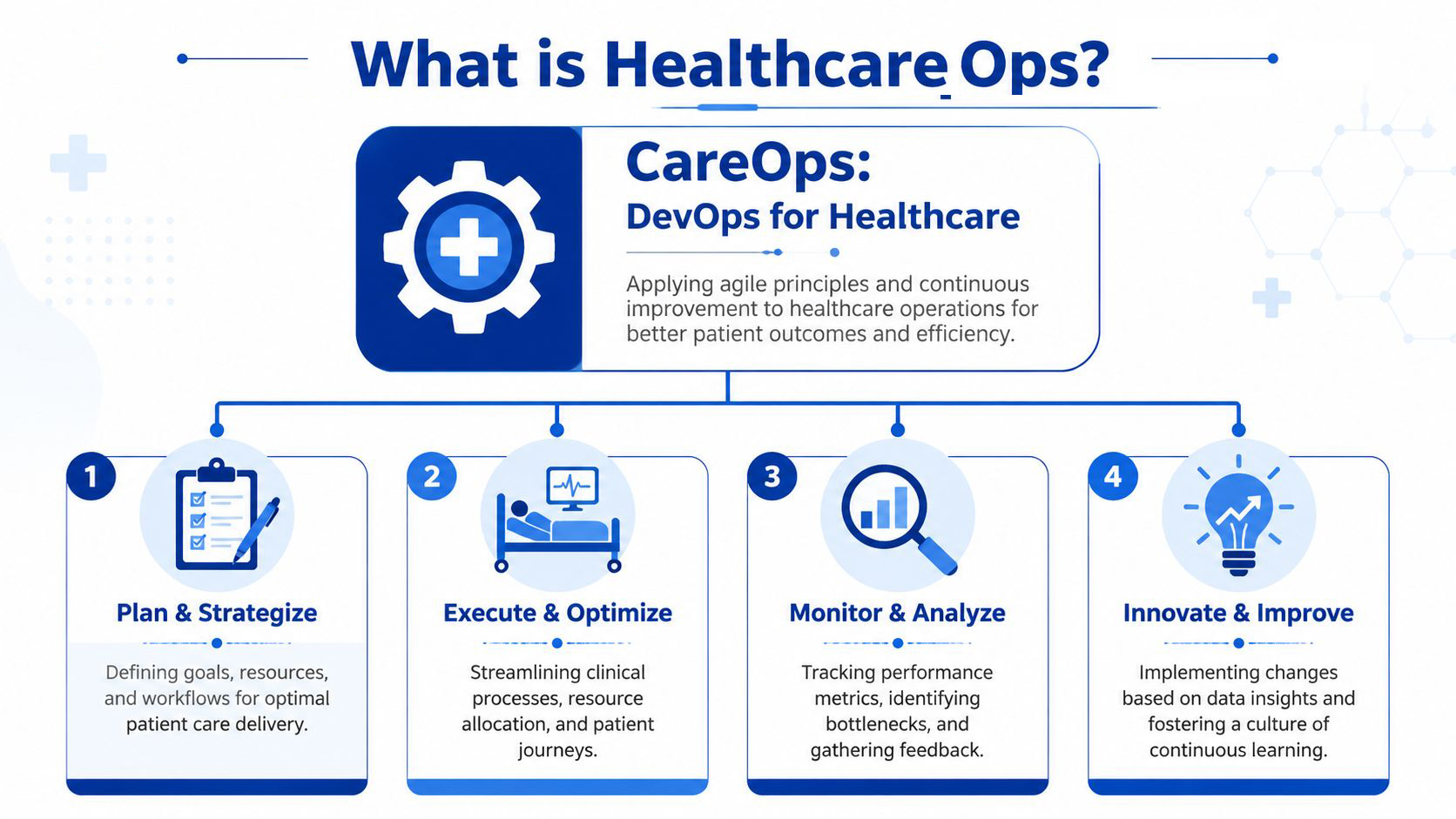
Three Ideas Sit at the Core
The first is cross-functional collaboration. A care pathway shouldn’t be redesigned only by IT or only by clinicians. It needs input from the people who run it day to day: physicians, nurses, clinic managers, operations leads, compliance staff, and product or engineering teams where technology is involved.
The second is automation of repeatable work. That doesn’t mean automating clinical judgement. It means reducing avoidable manual steps such as appointment reminders, intake routing, patient education messages, task assignment, or follow-up prompts after a visit.
The third is data-driven iteration. Instead of changing a process once a year and hoping for the best, CareOps teams monitor what’s happening and refine the workflow as they learn.
A Simple Analogy That Makes It Clearer
Think of a modern airport. Passengers don’t just need a plane. They need check-in, security, wayfinding, baggage handling, gate coordination, and real-time updates. Healthcare is similar. Clinical care is the aircraft, but operations determine whether anyone reaches the destination smoothly.
That’s why CareOps is bigger than software. Software is part of the answer, but the shift is operational. Teams agree on a pathway, define handoffs, choose the right metrics, and then use technology to support the process.
A related area many leaders overlook is billing and collections. If care delivery improves but payment workflows remain fragmented, the organisation still feels the strain.
CareOps works best when the team treats the patient journey as one connected system, not a series of departmental tasks.
What CareOps Is Not
It isn’t a single platform. It isn’t just another dashboard. It isn’t a rebranding of quality improvement, though it overlaps with it. And it isn’t only for large hospitals with enterprise budgets.
A small Canadian clinic can use HealthcareOps to tighten referral management, follow-up outreach, and documentation flow. A larger provider can use it to coordinate virtual care, remote monitoring, discharge pathways, and compliance controls across multiple teams. The scale changes. The logic doesn’t.
Key Benefits for Patients and Providers
CareOps matters because it changes daily work, not just strategy slides. The benefits show up in two places at once. Patients experience a more connected journey, and providers gain a more manageable operating model.
One industry benchmark points to why this matters. In 2024, a significant number of clinicians are reporting utilisation rates exceeding 66%, and in 2023, over 25% of care delivery was still mostly in-person, according to the State of CareOps 2022 post. When clinicians are already stretched, operational inefficiency becomes a clinical problem.
Clinical Benefits
For practitioners, the biggest gain is often reduced friction. When reminders, routing, and follow-up tasks are structured properly, staff spend less time hunting for information and more time acting on it.
That can improve care in practical ways:
Better continuity: Patients are less likely to disappear between assessment, testing, treatment, and follow-up.
Faster handoffs: Nurses, physicians, and coordinators see the same workflow state instead of rebuilding context each time.
Less cognitive overload: Teams don’t need to remember every next step because the system supports the sequence.
The patient also feels the difference. A care journey becomes clearer when messages are timely, instructions are consistent, and the next step is visible. That’s one reason digital engagement matters so much. This article on patient engagement technology in healthcare is helpful if you’re evaluating how portals, reminders, and messaging tools fit into a broader care model.
Business and Operational Benefits
Administrators usually care about reliability, cost control, compliance, and scale. CareOps helps with all four.
A well-run CareOps model can make it easier to standardise workflows without making care feel rigid. It can reduce duplicate effort, expose bottlenecks, and create a stronger audit trail. That’s especially important in Canada, where organisations often have to work across mixed systems, varying provincial processes, and strict privacy expectations.
Here’s the clearest contrast.
| Aspect | Traditional Model | CareOps Model |
|---|---|---|
| Care coordination | Staff rely on email, memory, and manual follow-up | Shared workflows guide the next action |
| Visibility | Teams see fragments of the patient journey | Teams work from a connected operational view |
| Improvement cycle | Changes happen slowly and reactively | Workflows are reviewed and refined continuously |
| Patient communication | Outreach is inconsistent and easy to miss | Messaging and follow-up are built into the process |
| Technology role | Systems store records but don’t drive action | Systems support execution, alerts, and measurement |
Why This Changes the Economics of Delivery
CareOps not only makes teams feel more organised. It changes how capacity is used. When a clinic reduces avoidable rework, clinicians can focus on higher-value tasks. When a hospital service line shortens delays between departments, it serves patients more predictably without demanding constant overtime or workarounds.
When a process is reliable, staff don’t need to compensate for it all day.
That’s the deeper benefit. CareOps turns operations into a lever for both patient outcomes and business performance.
The Architecture of a Modern CareOps System
Most healthcare organisations already have an EMR. The issue is that the EMR often acts as a record system, not an orchestration system. A modern CareOps setup builds around that foundation so data can move, tasks can trigger, and teams can see what’s happening across the care journey.
The Core Layers That Matter
Start with the system of record. In many Canadian settings, that’s the EMR or EHR. It holds encounters, orders, notes, diagnoses, and core patient information. CareOps doesn’t replace this layer. It makes it more operationally useful.
Next comes the integration layer, in which standards such as HL7 FHIR become important. FHIR makes it easier for scheduling tools, patient portals, analytics systems, remote monitoring platforms, and billing workflows to exchange data in a structured way. Without this layer, each new tool creates another silo.
Then comes the workflow layer, where operational logic lives. A referral arrives, a task is assigned, a missing lab result triggers outreach, or a no-show prompts rescheduling. These aren’t glamorous functions, but they’re what turn static records into active care delivery.
After that sits the analytics and monitoring layer. Teams need visibility into completion rates, delays, capacity, and patient movement across the pathway. If you’re looking at the broader technical foundations behind that data flow, this guide to healthcare interoperability solutions gives a useful overview.
Why Cross-Functional Design Matters
Technology alone won’t create a working architecture. The operating model has to be designed by the people who use it. That’s why team composition matters as much as the stack.
AI adoption in healthcare operations is at 55%, and teams that include clinicians, product managers, clinical operations, and engineers rose from 16% in 2023 to 36% in 2024, according to the State of CareOps 2024 report. The point isn’t that every organisation needs a large digital team. It’s that the best results come when care, operations, and technology solve the same problem together.
What This Looks Like in Practice
A modern CareOps system often includes:
EMR data feeds: Visit details, diagnoses, orders, and documentation.
Patient-facing tools: Portals, SMS reminders, forms, and education content.
Operational triggers: Rules for outreach, escalation, task routing, and missed-step detection.
Insight tools: Dashboards that show where journeys slow down or break.
The architecture should make the right action easier than the workaround.
That’s the standard worth aiming for. If staff still need side lists and separate trackers to keep care moving, the architecture isn’t complete yet.
Your Roadmap to Implementing CareOps
The organisations that succeed with CareOps rarely begin with a giant transformation programme. They start with one painful workflow, make it visible, and improve it in cycles. That approach is more realistic for a community clinic, and it’s often smarter for a larger provider too.
Start With One Pathway That Hurts
Pick a care journey where delays, handoff errors, or drop-offs are common. That could be referral intake, post-discharge follow-up, chronic disease management, or virtual visit preparation. The best pilot area is one where staff already know there’s friction and where improvement would be noticed quickly.
Write down the current path in plain language. Who receives the patient? What system do they use? Where does the next action depend on a phone call, memory, or spreadsheet? Such scenarios reveal hidden complexity.
Build the Team Before You Buy More Tools
CareOps needs operational ownership. A pilot team usually works best when it includes:
A clinical lead who understands the care pathway.
An operations lead who sees scheduling, staffing, and process issues.
A technical lead who can map integrations, workflow rules, and data capture.
A compliance or privacy voice if patient messaging, automation, or new data flows are involved.
This step matters because many healthcare projects fail in the gap between process design and technical build. CareOps closes that gap early.
Pilot, Measure, Refine
The strongest CareOps programmes don’t aim for perfection on day one. They launch a workable version, observe what happens, and improve the flow. That’s where the agile mindset matters.
High-performing organisations embed 70%+ of their care flows directly in-system, which cuts engineering dependency by 60% and enables weekly iterations, according to the State of CareOps 2023 report. That’s a major shift from older waterfall approaches, where teams wait months for changes.
A practical sequence often looks like this:
Map the baseline: Document the current workflow and identify failure points.
Design the first future state: Add only the changes that remove the biggest friction.
Launch a contained pilot: Use one clinic, one service line, or one patient segment.
Review real behaviour: Look at task completion, delays, missed follow-ups, and staff feedback.
Adjust quickly: Revise rules, forms, messages, and handoffs while the pilot is still active.
Small pilots reveal operational truth faster than large planning documents.
Scale What Proves Itself
Once a pilot works, don’t just copy and paste it everywhere. Turn it into a reusable operating pattern. Define which elements are standard, which need local variation, and which data fields or triggers must stay consistent across teams.
That’s how HealthcareOps becomes sustainable. Not by one big launch, but by repeatable improvement that staff trusts because they helped shape it.
Measuring Success With Key Performance Indicators
If CareOps can’t be measured, it won’t hold attention for long. Leaders need proof that workflow redesign is improving care, easing workload, or protecting margins. The best measurement approach is balanced. It tracks clinical performance, operational execution, and financial impact together.
Clinical KPIs
Clinical measures should show whether patients are completing the pathway and receiving more consistent care. Depending on the service, this may include adherence to follow-up schedules, timely care-plan completion, or patient-reported progress collected through digital tools.
The point isn’t to measure everything. It’s to choose indicators that reflect whether the redesigned pathway is helping patients move through care more reliably.
Operational KPIs
Operational indicators tell you whether the system is functioning as intended. Common examples include handoff completion, response time for follow-up tasks, rate of missed steps, and how often staff need manual workarounds.
Many organisations learn the most during this stage. A pathway may look clinically sound on paper, but still fail because a referral queue isn’t monitored, a message isn’t triggered, or one team has no visibility into the next step. For leaders building those reporting views, this guide on healthcare data analytics solutions is a strong reference point.
Financial KPIs
Financial indicators should answer a practical question. Is the organisation delivering care more efficiently without degrading quality?
A useful Canadian example comes from Ontario. In an Ontario value-based care pilot, a CareOps framework led to a 15 to 20% reduction in care drop-off rates and an average cost saving of $450 CAD per patient, as described in the CareOps metrics for the practice article. The reported savings were tied to task shifting and workflow optimisation within the EMR.
That example matters because it shows how operational design can affect both continuity and cost at the same time.
A Simple Scorecard Approach
Many teams do well with a short scorecard reviewed regularly:
One clinical measure: Did patients complete the intended care sequence?
Two operational measures: Where are delays or drop-offs occurring?
One financial measure: Is the redesigned pathway reducing waste or improving resource use?
Keep the scorecard small at first. A dashboard with too many metrics often hides the underlying story.
Good CareOps measurement answers three questions. Are patients moving through care? Are teams spending less effort on coordination? Is the model financially sensible?
Begin Your Journey to Connected Care
Healthcare leaders don’t need another abstract framework. They need a way to make care delivery more coherent. That’s what HealthcareOps offers. It brings operations into the same conversation as clinical quality, digital tools, compliance, and financial sustainability.
For a small clinic, that may mean fewer missed follow-ups and a more manageable staff workload. For a hospital department or virtual care provider, it may mean better handoffs, clearer ownership, and faster improvement cycles. In both cases, the gain is the same. Care becomes easier to run well.
The Canadian context makes this especially relevant. Providers are working within real access pressures, mixed digital maturity, and strict privacy expectations. That calls for operational models that are practical, interoperable, and adaptable. CareOps fits because it focuses on redesigning how care moves, not just adding another layer of software.
The best next step is usually modest. Choose one pathway. Bring the right people together. Map the current state accurately. Then improve the workflow in a way that staff can see and patients can feel.
Connected care doesn’t appear because a new platform is installed. It appears when teams align around a better operating system for delivery.
If your organisation is exploring secure, compliant, and scalable healthcare operations technology, Cleffex Digital Ltd can help you turn CareOps ideas into working systems. Their team supports healthcare providers, startups, and growth-stage organisations with custom software, interoperability, automation, and AI-driven solutions built around real operational needs.







