



A projected 5% to 10% reduction in annual healthcare system costs, equal to about $200 billion to $360 billion per year globally, is the kind of number that changes boardroom conversations from “Should we explore AI?” to “Where does intelligent automation fit in our operating model?” That estimate comes from a 2025 digital health trends report, and it matters in Canada because every health system is under pressure to improve access, productivity, and patient experience without compromising quality.
That's why intelligent healthcare systems deserve a more practical definition than the usual marketing language. They are connected clinical and operational systems that combine data, software, automation, and AI to help organisations make better decisions and remove friction from care delivery. In practice, that can mean faster documentation, better triage, more coordinated patient pathways, cleaner claims handling, and fewer manual handoffs between departments.
For Canadian hospitals, insurers, and clinic networks, the question isn't whether the technology is impressive. It's whether the system can work across fragmented records, provincial workflows, privacy constraints, and uneven digital maturity. That's where many initiatives stall.
The Dawn of Intelligent Healthcare
Boards often hear about AI in terms of diagnostics or futuristic patient journeys. The more immediate business case is less glamorous and more valuable. Reduce avoidable administrative load. Improve throughput. Support staff with better information at the point of decision.
An intelligent healthcare system isn't one product. It's an operating layer that sits across scheduling, records, monitoring, communication, analytics, and workflow automation. When it works, clinicians don't need to re-enter the same information in multiple tools, patients don't need to repeat their history at every transition, and administrators can act on live operational signals instead of stale reports.
What Makes a System “Intelligent”
The word “intelligent” gets overused. In healthcare, it should mean something specific:
It connects data sources so the right people can see the right information in context.
It analyses patterns in clinical or operational activity and turns them into actionable prompts.
It supports decisions and workflows instead of just storing information.
It improves over time as teams refine rules, interfaces, and governance.
That's a more grounded lens than treating AI as a standalone feature.
Intelligent healthcare systems create value when they remove operational friction first. Fully autonomous care can wait. Better coordination can't.
Canadian organisations also need to separate ambition from sequencing. A hospital doesn't need to launch advanced predictive models on day one. It often gets more return by improving documentation, referral flow, intake, discharge coordination, and patient communication first. Those areas are measurable, operationally visible, and easier to govern.
Why This Matters Now in Canada
Canada is well-positioned for this shift because healthcare is one of the country's largest and most digitisation-ready sectors. At the same time, provincial variation, legacy systems, and uneven interoperability make execution harder than the slide deck suggests.
A useful way to think about the market is this: the strategic opportunity is large, but the implementation burden is real. Leaders who want a broader view of the product space can look at the future of AI healthcare apps as part of their planning, but the winning programs usually start with one operational pain point and one accountable owner.
The Core Components of Intelligent Healthcare
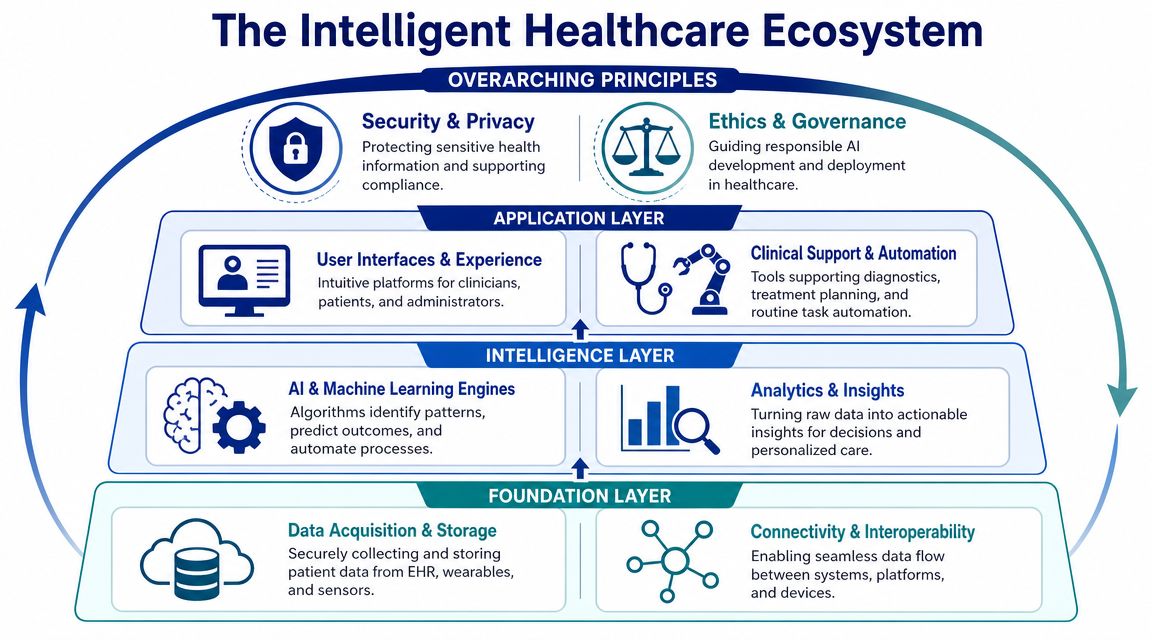
A good way to explain intelligent healthcare systems is to think of them as a digital central nervous system for a healthcare organisation. The sensors gather signals. The memory stores context. The brain interprets patterns. The hands carry out actions through workflows, alerts, and user interfaces.
That architecture matters because many failed projects focus on one layer only. They buy an AI tool without fixing the data flow or deploy remote monitoring devices without integrating the readings into clinician workflows.
The Senses, Memory, and Brain
At the edge of the system are the “senses”. These include wearables, bedside devices, patient apps, intake forms, call centre transcripts, scheduling platforms, and claims systems. They generate signals about patient status, utilisation, risk, and workflow bottlenecks.
The next layer is “memory”. That includes EHR or EMR platforms, data warehouses, cloud environments, document repositories, and identity systems. This layer doesn't just store data. It determines whether information is structured, accessible, secured, and usable across settings.
The “brain” sits above that foundation. AI and machine learning models analyse patterns, support triage, draft summaries, flag missing information, route tasks, and prioritise work queues. Analytics tools then make this visible to humans through dashboards, alerts, and embedded workflow guidance.
Here's the architecture in one view:
Why Interoperability Is the Hard Part
In Canadian deployments, the main technical constraint isn't model quality. It's an interoperability architecture. Wearable sensors and body-area networks can generate continuous physiological streams such as ECG, SpO2, and blood pressure, but those signals only become operationally useful when they're fused with EMR data for structured analysis. The literature notes that this sensor-to-EMR integration remains challenging, even though it's essential for autonomous decision support and real-time telemonitoring, as described in this research on intelligent healthcare architecture.
That point has practical implications:
Device data without workflow integration creates more noise, not more value.
AI outputs without a record context are hard for clinicians to trust.
Remote monitoring without escalation rules becomes another inbox no one owns.
What Actually Works in Implementation
The strongest programmes treat architecture as a service design problem, not just an IT problem. They decide early where data should originate, who validates it, where it should surface, and what action should follow.
For many organisations, the first useful automation sits in access and administration. If your team is evaluating patient-facing workflow tools, this guide to virtual medical receptionists is a helpful example of how AI can support front-desk coordination, intake, and communication without pretending to replace core clinical judgment.
A practical build sequence usually looks like this:
Connect the core systems first. Start with EMR, scheduling, identity, and messaging.
Define one workflow owner. Every automated alert or handoff needs an accountable team.
Embed outputs where staff already work. Don't make clinicians open another dashboard.
Design for exceptions. Escalations, overrides, and audit trails matter as much as the model.
Organisations planning broader integration often need platform-level thinking rather than point solutions. That's why many leaders start with a view of connected healthcare platforms before selecting specific AI tools.
Transforming Patient and Business Outcomes
Administrative waste still consumes a meaningful share of healthcare spending, and that is why intelligent healthcare gets broad attention. The strongest business cases do not start with abstract innovation goals. They start with a measurable operational problem that affects cost, access, experience, or all three.
For Canadian providers and payers, the opportunity is real, but so are the constraints. Data often sits across hospital systems, insurer workflows, regional repositories, and provincial programmes that were not designed to work as one operating model. Intelligent healthcare creates value when it closes those gaps in a way staff can use, while respecting privacy obligations, procurement limits, and equity concerns for patients who are harder to reach through digital channels.
Where Providers and Insurers See Value
Providers usually get the earliest returns in places where time is being lost every day. Documentation support, intake routing, referral coordination, discharge operations, and patient communication can reduce avoidable delays without asking clinicians to change their judgment. The gain is practical. Less manual handling. Fewer dropped handoffs. Better use of scarce staff time.
Insurers and health plans look at a different operating problem. Claims review, prior authorisation, fraud detection, provider communication, care management outreach, and risk stratification all depend on cleaner information flow and fewer exceptions. In that setting, intelligent systems improve consistency first. Savings follow when rework, unnecessary escalation, and avoidable service friction start to decline.
The point for Canadian organisations is not to chase every new tool entering the market. It is to choose use cases where fragmented data, provincial process variation, and service inequities are already creating a visible cost.
Intelligent Healthcare Application Benefits
| Application Area | Primary Benefit for Providers | Primary Benefit for Insurers | Key Metric Improved |
|---|---|---|---|
| Clinical documentation | Less clinician admin burden and better chart completion | Clearer supporting information for downstream review | Documentation turnaround |
| Intake and triage | Faster routing to the right service line | Better member navigation and earlier case identification | Time to first response |
| Care coordination | Fewer missed handoffs across settings | Better continuity across covered pathways | Transition reliability |
| Remote monitoring | Earlier visibility into patient deterioration | Stronger chronic care oversight | Alert response workflow |
| Claims and authorisation | Fewer back-and-forth requests with payers | More consistent adjudication and reduced manual review | Processing cycle time |
| Member or patient communication | Better follow-up and fewer missed instructions | More timely outreach and service updates | Engagement completion |
| Revenue integrity | Cleaner coding support and fewer administrative leaks | Better validation of submissions and payment logic | Rework volume |
ROI Comes From Workflow Redesign
Most failed AI projects in healthcare do not fail because the model is weak. They fail because no one changed the process around it. If an alert lands in a queue without an owner, or if a recommendation arrives outside the system where staff already work, the organisation pays for intelligence and gets more operational noise.
Board-level test: If a team can't name the current bottleneck, baseline the manual steps, and identify who acts on the AI output, they're not ready to buy the tool.
The first metrics to track are operational. Turnaround time, rework volume, documentation completeness, first-pass resolution, staff hours returned to patient-facing work, and escalation rates give a clearer view of value than broad promises about transformation. Clinical improvement often appears later, after the workflow has been configured properly and staff trust the output.
This matters even more in Canada, where one deployment may need to fit different privacy interpretations, reimbursement rules, and referral pathways across provinces. A solution that performs well in one health system can struggle in another if consent models, integration standards, or service access assumptions are different. Strong implementation teams address those trade-offs early instead of discovering them after rollout.
Hospitals dealing with denials, underpayments, and administrative leakage should connect intelligent automation to financial operations as well as care operations. If your team is trying to master healthcare revenue recovery, the same discipline applies. Fix the handoff points, define accountability, and measure where revenue is being lost before adding more technology.
Teams comparing vendors should also review AI-powered healthcare solutions for providers and payers with a strict operating lens. The right purchase is the one that removes friction from a high-cost workflow, fits Canadian governance requirements, and produces a result your finance, operations, and clinical leaders can all verify.
Intelligent Healthcare in Action
Concepts become useful when they show up in day-to-day operations. The most convincing intelligent healthcare systems aren't dramatic. They make ordinary work less fragmented.

A Hospital Discharge Team That Stops Guessing
A Canadian hospital wants to reduce avoidable readmissions and improve discharge quality. The problem isn't that staff lack commitment. The problem is that risk signals sit in different places. Clinical notes are in one system, medication changes in another, social support indicators in another workflow, and follow-up booking status in a separate queue.
The intelligent solution isn't “replace the EHR”. It's to create a discharge support layer that pulls those signals together, flags patients who need closer follow-up, and pushes a structured task list to the discharge coordinator and community care team.
What changes in practice?
Nurses and care coordinators see which discharge elements are incomplete.
Physicians get a clearer summary before sign-off.
Post-discharge teams receive alerts tied to actual handoff tasks, not generic referrals.
The measurable result in this type of deployment is usually operational before it is clinical. Teams spend less time hunting for information, fewer steps fall between settings, and follow-up work becomes more consistent.
An Insurer That Fixes the Queue, Not Just the Algorithm
An insurance organisation faces a claims backlog. Not every claim is complex, but every file enters the same administrative pathway. Staff spend too much time on repetitive validation and too little on the claims that require judgment.
A practical intelligent system classifies incoming claims, extracts structured fields, checks for missing elements, and routes straightforward submissions into a fast review path while escalating ambiguous cases to experienced staff. That doesn't eliminate human review. It protects it.
The biggest gain is often queue discipline. Claims staff stop treating every file as equally urgent. Managers can see where work is stalling. Member communication becomes more predictable because the system can trigger status updates when the workflow changes state.
The best automation in claims is selective. It accelerates routine work and preserves human attention for exceptions, disputes, and edge cases.
A Rural Clinic Network That Uses Telemonitoring Properly
A network of rural clinics wants to support patients with chronic conditions between visits. The obvious idea is remote monitoring, but device rollouts often fail when readings arrive without context or ownership.
A stronger model combines home-based readings with threshold rules, care-team routing, and patient communication. A nurse doesn't need every datapoint. The nurse needs a clear signal that someone's pattern needs review and a way to respond within an agreed workflow.
That matters in geographies where in-person access is harder, and continuity depends on coordination rather than proximity. It also turns telemonitoring into part of routine care instead of a parallel experiment.
For teams building clinical knowledge workflows around evidence and documentation, tools such as AI for healthcare researchers can also support review and synthesis tasks around medical literature. Used carefully, that kind of support is most valuable when it shortens research and preparation time for clinicians, analysts, and programme teams.
Navigating Implementation and Governance
Most intelligent healthcare initiatives don't fail because the idea is wrong. They fail because governance shows up too late. By the time leaders start asking who owns the data, how consent works, what the fallback process is, or whether the workflow is equitable, the purchasing decision has already outrun operational reality.
In Canada, this issue is sharper because healthcare data is siloed across primary care, hospitals, and community settings. AI is only as useful as the interoperability layer beneath it, and data integration plus cybersecurity are prerequisites for supporting patient pathways reliably, as discussed in this Canadian perspective on intelligent healthcare.
Governance Has To Start Before Procurement
If a vendor demo begins with model sophistication and ends without a discussion of integration, privacy, and workflow ownership, that's a warning sign. A healthcare organisation should know before procurement how the system will fit into existing decision rights and operational controls.
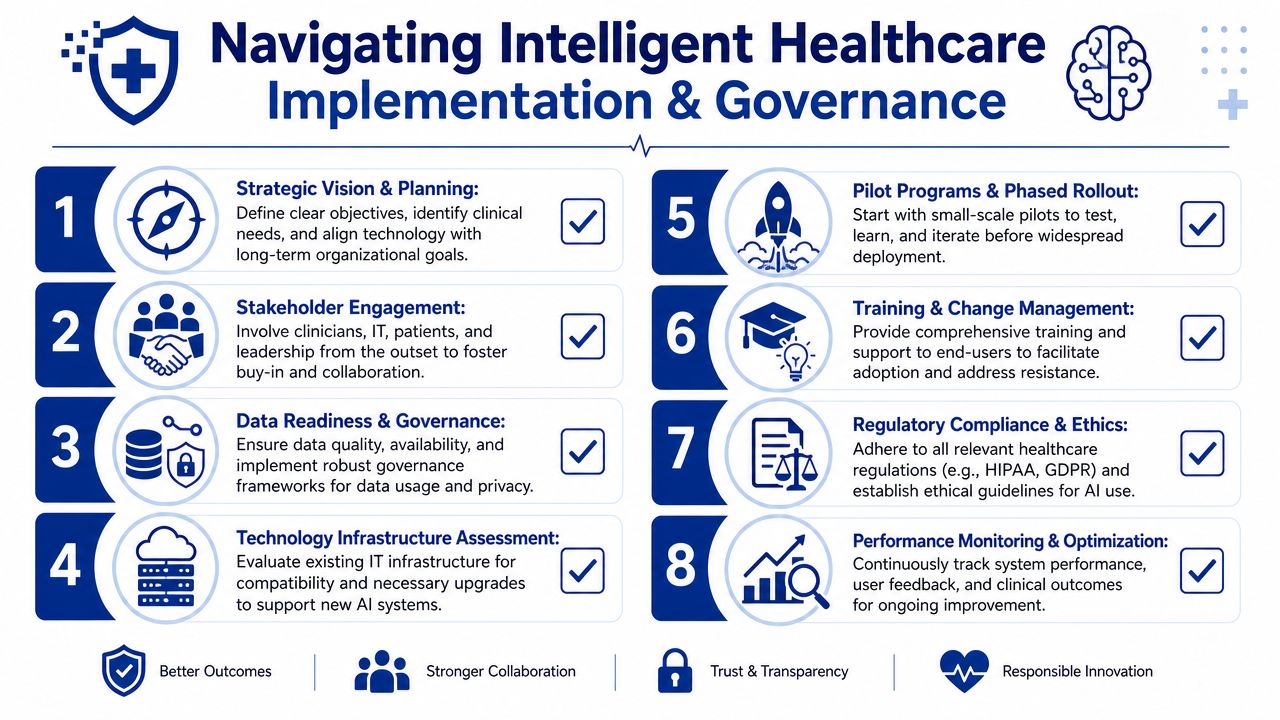
This governance checklist captures the essentials:
The Canadian Implementation Priorities
Leaders usually need to work through five issues in order.
Data Access and Quality
If patient records are incomplete, duplicated, or locked in departmental silos, AI won't repair that on its own. Integration strategy comes first.Workflow Ownership
Every alert, recommendation, or generated summary needs a named owner. If no one owns the action, the tool becomes background noise.Privacy and Security
Sensitive health information demands role-based access, auditability, secure architecture, and clear data handling rules. This is not optional.Procurement Fit
Provincial and organisational procurement models differ. The vendor needs to fit your contracting reality, not just your technical wishlist.Change Management
Clinicians and administrative teams adopt systems when they save time in real tasks. They resist tools that add screens, duplicate entry, or unclear accountability.
Equity Isn’t a Side Note
One of the most under-addressed questions is who benefits first. AI can help surface high-risk patients and personalise interventions, but only if organisations invest deliberately in equitable infrastructure, diverse data, and community participation. Otherwise, intelligent systems can reinforce language, racial, and geographic disparities, as argued in this health equity discussion on AI and underserved communities.
That means equity should show up in implementation decisions, not just strategy statements:
Validate across populations. Test workflows and outputs against different demographic and regional contexts.
Include underserved settings early. Don't design only for tertiary hospitals with stronger digital infrastructure.
Review language and access barriers. Patient communication workflows need to work for real communities, not ideal users.
Measure burden distribution. Check whether the tool reduces workload broadly or shifts it onto already stretched teams.
A system that works well in one urban hospital but fails in rural clinics or community care isn't ready for scale in Canada.
For organisations choosing build partners, delivery experience is paramount. Cleffex Digital Ltd is one example of a Canada-based software development company that works on custom healthcare software and integration-focused digital solutions. The relevant question isn't branding. It's whether a partner can work inside healthcare constraints, integrate with existing systems, and support phased implementation rather than selling a generic platform story.
The Future and How To Choose Your Partner
Health system spending is under pressure across Canada, while expectations for access, service, and reporting keep rising. In that environment, delaying intelligent healthcare initiatives has a cost. Organisations that wait too long often end up paying more later through rushed procurement, weak integration choices, and tools that solve a narrow problem but add operational burden elsewhere.
The next phase of the market will reward disciplined buyers, not early adopters for their own sake. The strongest returns are coming from targeted applications with a clear operating owner: ambient documentation, prior authorisation support, patient communication, coding assistance, and workflow orchestration across fragmented systems. Fully autonomous care remains a limited fit for most Canadian organisations, especially where data is spread across departments, vendors, and provincial platforms.
Canadian healthcare leaders should expect the partner market to get noisier before it gets better. More vendors will claim healthcare capability. Fewer will be able to show they can handle PHIPA or other provincial privacy requirements, hospital security review, procurement cycles, bilingual or multilingual patient communication needs, and integration with existing clinical and administrative systems.
What To Look For in a Technology Partner
Choose partners that can do three things well:
Work with your actual data environment. That includes incomplete records, legacy systems, inconsistent standards, and different levels of digital maturity across sites.
Deliver within Canadian operating constraints. Provincial regulation, privacy review, cybersecurity controls, data residency, and public-sector procurement should be part of the plan from day one.
Design around frontline workflows. Clinicians, operations leaders, and IT teams should shape the process together so the tool reduces effort instead of adding another layer of clicks, exceptions, and manual checks.
A credible partner will spend less time selling model sophistication and more time explaining integration scope, change management, fallback procedures, human review, consent handling, and post-launch measurement. That is usually the difference between a pilot that photographs well and a system that improves throughput, documentation quality, or patient access.
For organisations choosing build partners, delivery experience matters more than product positioning. Cleffex Digital Ltd is one example of a Canada-based software development company that works on custom healthcare software and integration-focused digital solutions. The practical question is whether a partner can work inside healthcare constraints, connect with existing systems, and support phased implementation that produces measurable value.







