



You're likely in one of two situations right now. You either have a sharp healthtech idea and you're trying to figure out how to build it without getting buried by compliance, or you've already spoken to a few software shops and realised the quotes, timelines, and legal language don't look anything like a normal startup app.
That confusion is justified.
A patient-facing symptom tracker, a clinic workflow tool, and a telemedicine platform may all look like “apps” from the outside. They are not built under the same rules. In healthtech, the product has to earn trust from users, clinicians, buyers, privacy officers, and sometimes regulators before it earns growth. If your MVP handles personal health information, the foundation matters more than the polish.
Canada is a strong place to build right now, but only if you approach it with discipline. Canadian startups raised CAD $1.26 billion in Q1 2025, with over CAD $800 million specifically flowing into MVP-focused ventures. That tells me two things. Capital is still backing lean product validation, and founders who ship focused MVPs still have an opening.
The mistake is thinking “lean” means “cheap and loose”.
In healthtech, lean means narrow feature scope, not relaxed security, weak consent flows, or vague integration planning. If you're building for Canada first, and you want the option to expand across North America, your architecture, contracts, and vendor choices need to reflect that from day one.
Your HealthTech Vision Meets Reality
A first-time founder usually starts with the same assumption. Build a simple version, get users, then clean up compliance later. That works in plenty of sectors. It's reckless in healthcare.
If your product touches appointment data, clinical notes, patient messages, intake forms, or insurer-facing evidence, your MVP isn't just a test product. It's the beginning of a regulated system. That changes everything from your cloud setup to your database structure to the questions you ask in vendor interviews.
Where founders get stuck
Most founders don't fail because the idea is weak. They fail because they underestimate what “viable” means in healthcare.
A viable healthtech product has to do more than demonstrate demand. It has to be safe to use, clear about consent, reliable under real workflows, and structured well enough that you don't need a painful rebuild before your first pilot. In Canada, that also means you can't blindly follow a U.S.-only playbook and hope it translates.
Practical rule: In healthtech, the fastest route is usually the one with the least rework, not the one with the lowest first quote.
The opportunity is real, but so is the filter
The Canadian market isn't short on appetite for software-led validation. The funding numbers above make that obvious. But healthcare buyers don't reward speed alone. They reward products that can survive due diligence.
That's why healthtech MVP development services matter. A proper team doesn't just code screens. They define the smallest compliant product that can prove the business case without creating technical debt you can't afford later.
Founders who get this right usually make three early decisions well:
They narrow the use case hard: One workflow, one user group, one core outcome.
They define compliance scope early: Not with hand-waving, but with actual data flow mapping.
They choose a vendor that understands Canadian health privacy: Not a generalist app team learning on your budget.
That discipline feels slower at the start. It usually saves time where it matters, during pilot readiness, enterprise review, and procurement.
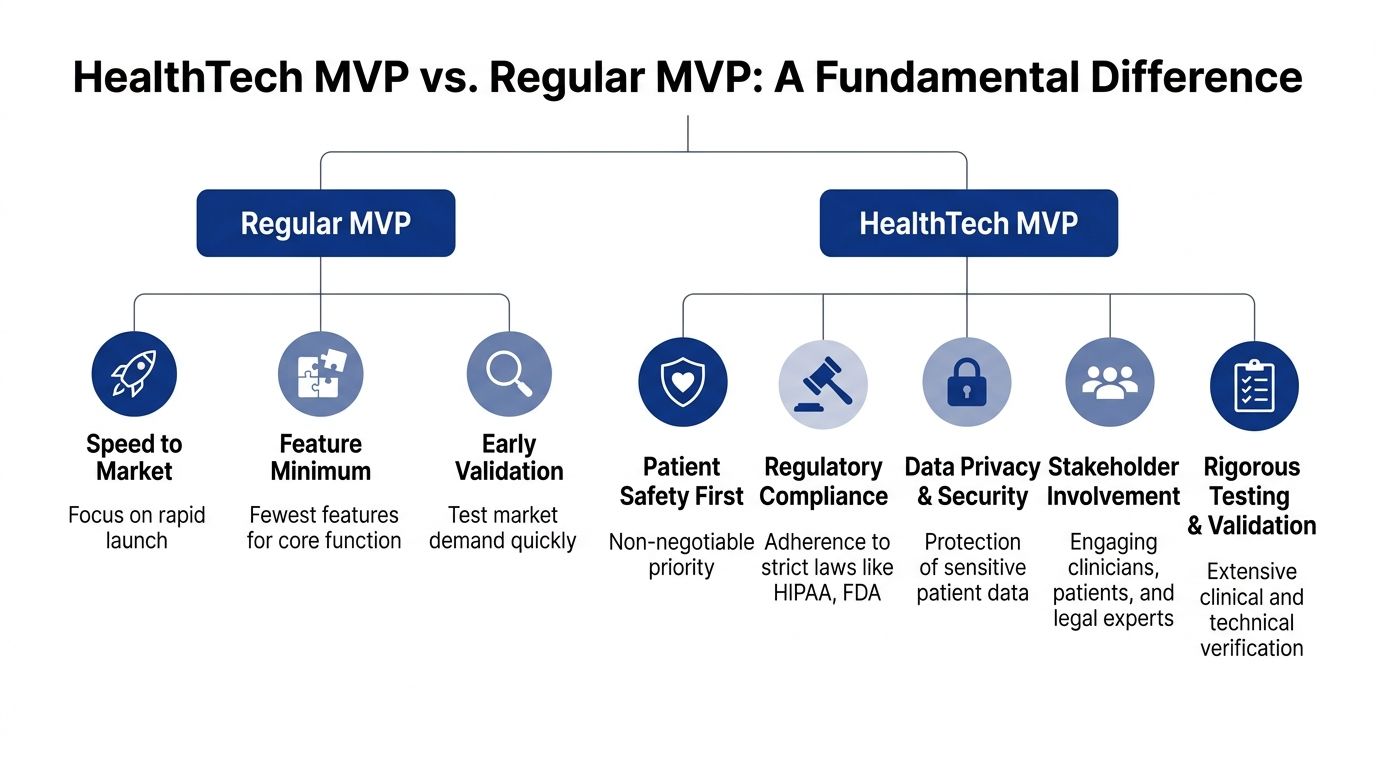
Why a HealthTech MVP Is Not a Regular MVP
Most startup advice gets the first word wrong. In healthtech, “minimum” applies to features. It does not apply to privacy controls, auditability, or data integrity.
A regular MVP can be rough around the edges if it proves demand. A healthtech MVP can't take that shortcut. If the system stores sensitive data, logs user activity poorly, or mixes protected data with general application logic, you haven't built an MVP. You've built future rework.
The house analogy founders actually understand
Think of a normal MVP as a cabin. It needs to stand up, keep out the weather, and let people use it.
A healthtech MVP is closer to a safe house. The walls still matter, but the hidden systems matter more. You need secure entry, controlled access, logs of who entered, proper separation between rooms, and infrastructure that holds up under inspection. If you skip that and promise to retrofit later, you'll tear into the structure you already paid for.
That's why a generic agency often underestimates healthcare work. They scope visible features and ignore the invisible obligations.
Canada-first changes the architecture
Here's the gap I see constantly. Founders read U.S.-centric advice, hear “HIPAA-compliant,” and assume that's the whole brief. It isn't.
Most healthtech MVP guides over-index on U.S. HIPAA compliance while leaving Canadian startups unclear on how PIPEDA and provincial laws such as Ontario's PHIPA change MVP architecture, data residency, and consent flows, as noted by Digital Health Canada's discussion of why an MVP comes first in healthcare.
That single point has major consequences:
Consent flow design changes: You need language, UX, and records that fit Canadian expectations.
Data handling choices change: Storage, access, and segregation have to reflect Canadian privacy obligations.
Vendor selection changes: A team that only knows HIPAA checklists may miss what matters for a Canadian deployment.
A healthtech MVP isn't “small software for healthcare.” It's a constrained product built on full-strength foundations.
What “viable” should mean
Use this test before approving any proposal for healthtech MVP development services:
| Question | Weak answer | Strong answer |
|---|---|---|
| How is PHI separated? | “We'll secure the database” | Clear service boundaries and data segregation plan |
| How are consent flows handled? | “We'll add terms later” | Consent logic is mapped into onboarding and data use paths |
| How are audit trails managed? | “We log key actions” | Role-based logging tied to sensitive events and access history |
| How is future integration planned? | “We can add APIs later” | Interoperability assumptions are defined before core build |
If a vendor treats compliance as documentation instead of architecture, walk away.
Navigating the North American Compliance Maze
Founders don't need to become lawyers. They do need to understand enough to stop making expensive product decisions with incomplete assumptions.
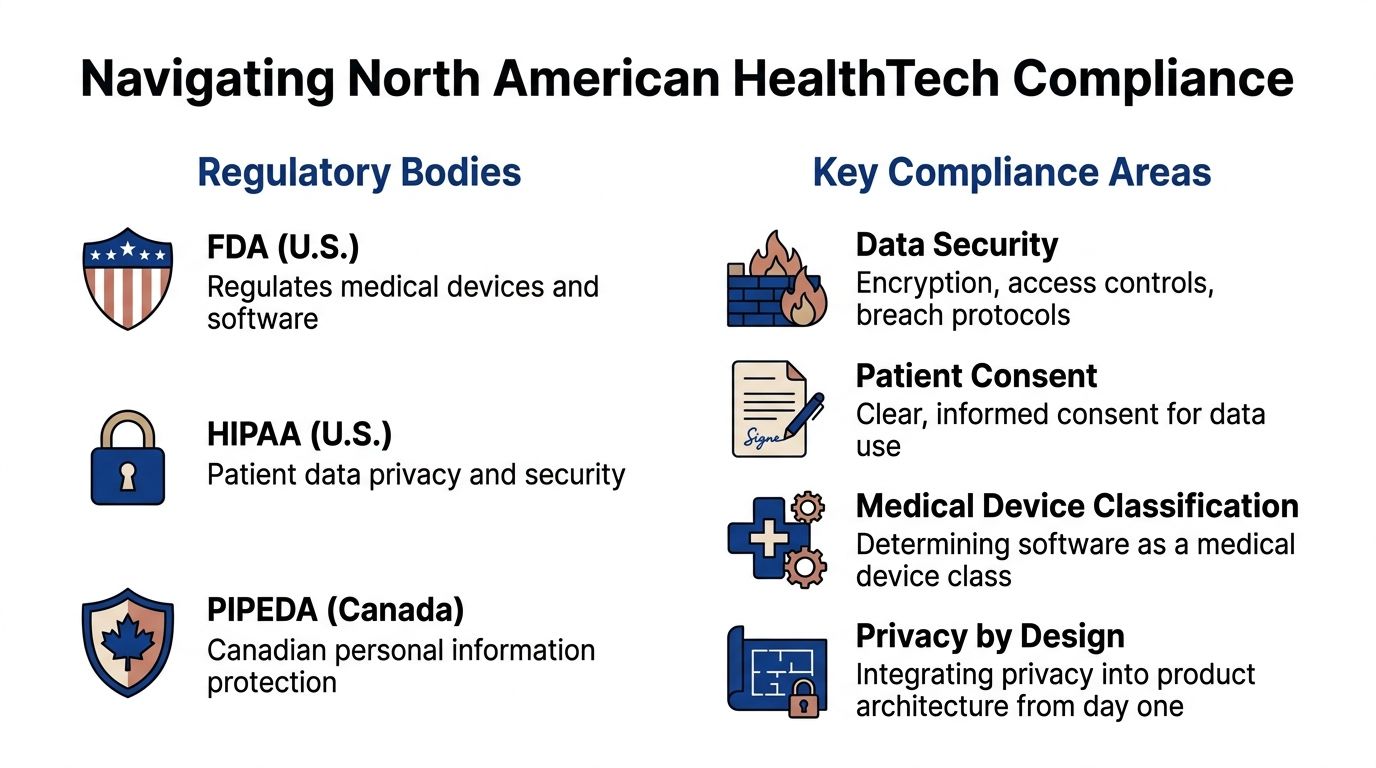
In North America, the practical compliance question is simple. What rules shape your system if you launch in Canada, or build in Canada with U.S. expansion in mind? For most startups, that means thinking about PIPEDA, relevant provincial rules such as PHIPA in Ontario, and HIPAA when U.S. data flows, or partners enter the picture.
What this means in product terms
You don't build a compliant product by adding a policy page. You build it by making architecture choices that support lawful data use.
In the Canadian healthtech MVP context, architecture must embed HIPAA/HITECH-aligned controls from the first commit, because Canadian privacy laws such as PIPEDA require comparable safeguards, and failures to isolate sensitive services create direct liability. Data breaches can trigger mandatory reporting and fines of up to $100,000 per violation under federal law, according to Bridge Global's healthtech MVP development guidance.
That should drive immediate technical decisions:
Separate protected data early: Don't let PHI sprawl across services.
Define tenant boundaries: Especially if you serve multiple clinics or organisations.
Enable audit logging from the start: Not after launch.
Provision cloud environments with compliance settings already in place: AWS and Azure both support this when used properly.
A simple comparison founders can use
| Framework | Where it matters most | What founders should care about |
|---|---|---|
| PIPEDA | Canada federal context | Consent, safeguarding personal information, accountable handling |
| PHIPA | Ontario health information context | Health-specific privacy obligations and operational handling rules |
| HIPAA | U.S. healthcare ecosystem | Security, privacy, and vendor responsibility in U.S. workflows |
The biggest mistake is treating these as separate legal boxes with no technical implications. They shape your user permissions, storage model, logging, vendor contracts, and incident response planning.
Don't forget accessibility
Privacy isn't the only requirement that belongs in the architecture. If your users are patients, clinicians, or caregivers, accessibility affects adoption, risk, and trust. A practical primer on accessibility in healthcare is worth reviewing before design starts, especially if your product includes intake, consent, messaging, or results review.
A lot of founders leave accessibility to the design QA stage. That's too late. Colour contrast, keyboard navigation, readable form patterns, and plain-language consent affect whether people can use your product safely.
What to ask your vendor before any contract
Use these questions in your first serious call:
How do you separate PHI from general application services?
How do you handle audit logging for access and data changes?
What Canadian privacy assumptions are built into your default architecture?
How do you document vendor responsibilities when U.S. HIPAA obligations also apply?
What secure cloud controls do you enable at provisioning, not later?
If you need a useful technical primer for the U.S. side of the equation, this HIPAA-compliant healthcare software guide gives founders a practical view of the software obligations involved.
Compliance work that starts after design usually ends with redesign.
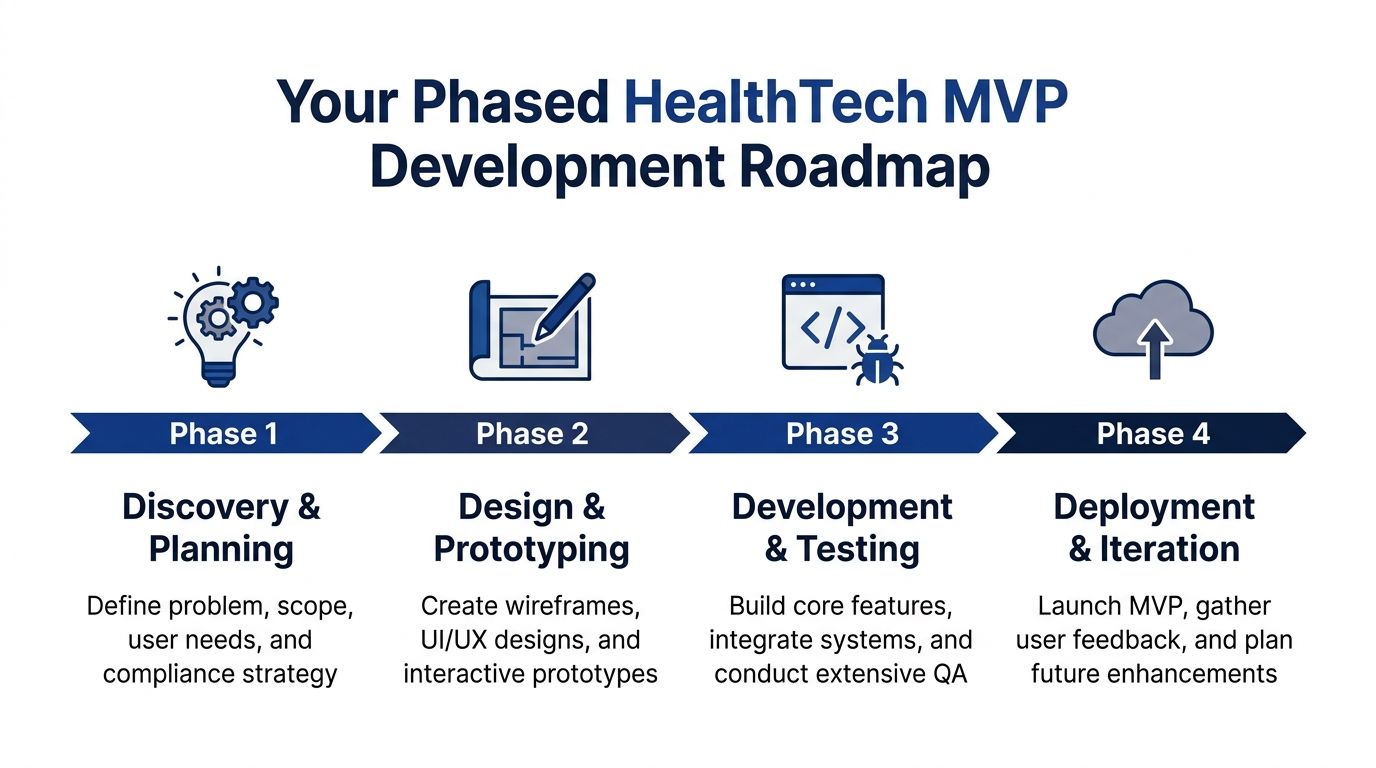
A Phased Development Roadmap for Your MVP
Good healthtech MVP development services don't begin with coding. They begin with decisions that remove ambiguity. If your team starts by debating frameworks before defining data flows, user roles, and pilot conditions, the project is already drifting.
The build should move in phases, but not in silos. Design, engineering, compliance, and workflow validation need to overlap enough to catch bad assumptions early.
Phase one through two
The first phase is discovery and planning. In this phase, founders need to be ruthless. Define the user, the core workflow, the minimum dataset, the regulated data touchpoints, and the pilot environment. If those aren't explicit, every later estimate is fiction.
The second phase is design and prototyping. In healthcare, UI work isn't decoration. It's where trust, clarity, and safe task completion start. Intake flows, alerts, permissions, and consent screens should be validated in prototype form before development moves far.
A broader product lifecycle stages guide is useful here because it forces founders to think beyond the first release and connect MVP decisions to long-term product maturity.
Phase three is where most mistakes get expensive
Development should focus on the narrowest production-worthy version of the product. That means real authentication, proper logging, clean data models, and tested permissions. Not placeholder security.
This is also the phase where integration assumptions need to become concrete. If your future includes provider systems, billing systems, or payer workflows, your engineers should design with that future in mind even if the first release uses a limited interface.
Use this working sequence:
Build core workflows first: Registration, intake, messaging, scheduling, documentation, or whatever solves the central pain.
Implement role-based access early: Don't wait until QA to think about who sees what.
Test against realistic data conditions: Missing fields, duplicate records, interrupted sessions, partial forms.
Review logs and permissions continuously: Security isn't a final sprint task.
If you're evaluating technical execution patterns, this guide to building secure healthtech applications is a practical reference for founders who want to ask better engineering questions.
Phase four determines whether the MVP is usable
Deployment is not the finish line. In healthtech, it's the start of scrutiny.
A sensible MVP launch usually means a limited pilot, controlled user groups, monitored support channels, and clear issue triage. You want to learn from real use without exposing the product to uncontrolled risk. That means preparing operationally, not just technically.
Launch a smaller pilot than your ego wants. You'll learn more, and you'll break fewer things that matter.
The founder's role in each phase
| Phase | Founder's job |
|---|---|
| Discovery | Decide what problem you are actually solving |
| Design | Protect simplicity and approve only essential workflows |
| Development | Hold the line on scope and require visibility into security decisions |
| Deployment | Collect feedback from real users, not just internal champions |
Founders often disappear after kickoff and resurface at demo time. That's a mistake. Your job is to keep the product honest, focused, and useful.
Budgeting for Your HealthTech MVP
At this juncture, founders either get realistic or get hurt.
If you compare healthtech quotes to generic SaaS quotes, healthtech will look expensive. It is expensive. The relevant question isn't whether it costs more. The relevant question is whether the quote reflects the actual work required to launch something usable and compliant.
What the market data says
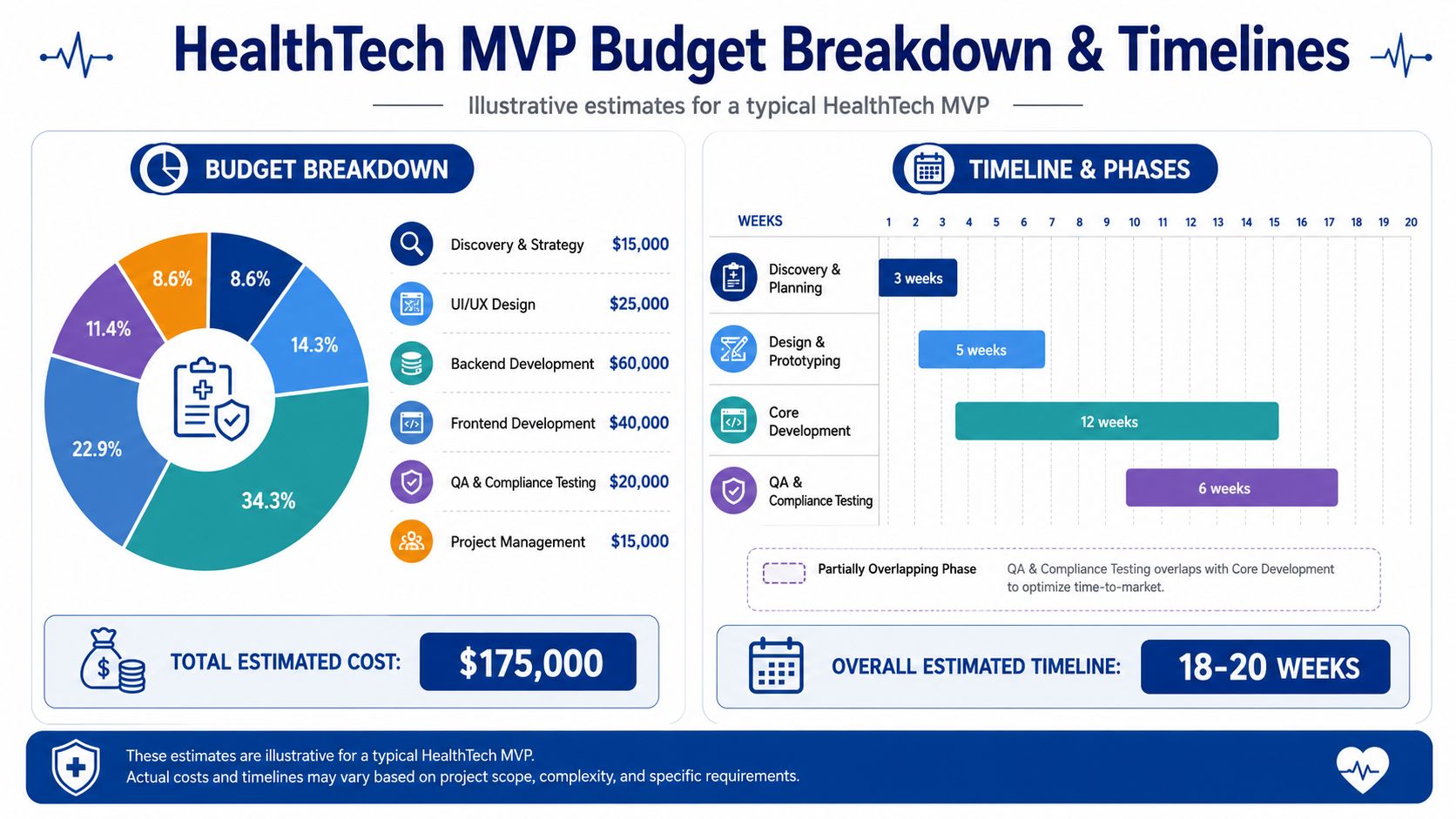
In Canada, healthtech MVPs cost 1.5x to 5x more than comparable non-healthcare applications. The same source notes that a wellness app MVP typically ranges from $50,000 to $150,000, while a HIPAA-compliant telemedicine or EHR-integrated product usually requires $150,000 to $350,000. For medical devices requiring certification, the budget can rise to $500,000 or more, according to Momentum's analysis of healthtech MVP cost in Canada.
Those ranges make sense. You're not just paying for screens and APIs. You're paying for compliance-aware architecture, secure infrastructure, auditability, testing discipline, and integration planning.
Why one quote can be wildly higher than another
The big cost drivers are usually these:
Compliance baseline work
Access controls, audit logs, secure cloud configuration, data segregation, and consent handling all take time before flashy features even begin.Integration complexity
EHR, EMR, FHIR, HL7, identity providers, scheduling systems, and insurer workflows all raise cost because they raise uncertainty and validation effort.Clinical workflow design
A product that fits how clinics or patients work takes more discovery and more iteration than a generic consumer app.Certification path
If your product edges toward regulated device territory, budget pressure rises quickly.
A useful budgeting lens
Think in three buckets, not one lump sum.
| Budget bucket | What belongs there |
|---|---|
| Foundation | Discovery, architecture, compliance baseline, secure cloud setup |
| Build | Core user flows, backend, frontend, integrations, testing |
| Readiness | Pilot prep, monitoring, support process, fixes after first live usage |
This helps you avoid the classic founder error of spending too much on visible features and too little on infrastructure.
Where AI and third-party tools can distort estimates
A lot of founders now want AI in version one. Sometimes that's justified. Often it isn't.
If your MVP includes external AI or computer vision services, pricing can become harder to forecast because usage costs don't behave like one-time build costs. Before approving those dependencies, it helps to understand Vision platform costs or any similar usage-based tooling model so you don't commit to a feature that makes your pilot economics messy.
Cheap healthtech builds usually aren't cheap. They simply move the bill to the rebuild phase.
My budgeting advice
If you're early, budget for one sharp use case and one credible pilot. Don't budget for your eventual platform story.
If a vendor promises a broad healthtech platform on a low-end app budget, they're either leaving out critical work, or they don't understand the category. Neither option helps you.
Choosing Your Expert Development Partner
Your development partner will shape your MVP's risk profile, delivery speed, and compliance posture long before users judge the feature set.
In HealthTech, a vendor is not just writing code. They are making architecture decisions that affect where personal health information sits, how consent is handled, what gets logged, and how painful your first pilot becomes. For a Canada-first product, that starts with PIPEDA and the provincial rules that apply to the health data you collect, store, or transmit. If a team treats those as paperwork for later, remove them from the shortlist.
Start by testing judgment.
A credible HealthTech partner should explain, in plain language, how they classify sensitive data, choose hosting regions, set up role-based access, manage audit logs, and prepare for later integrations with provider systems. They should also understand that Canadian requirements can force different product and infrastructure choices than a US-only HIPAA build. If you want a founder-focused benchmark for that evaluation, this healthcare technology partner in Canada guide is a useful reference.
Use a shortlist scorecard that focuses on execution, not sales polish:
| Evaluation area | What you want to hear |
|---|---|
| HealthTech delivery history | Specific examples involving patient, provider, payer, or regulated workflows |
| Canada-first privacy understanding | Working knowledge of PIPEDA and the provincial rules relevant to your launch market |
| Security ownership | Clear answers on cloud setup, access controls, logging, backups, and incident response |
| Architecture discipline | A documented discovery process, data flow mapping, and realistic scope control |
| Interoperability planning | Experience designing for FHIR, HL7, or future EHR integration without overbuilding version one |
| Pilot readiness | A plan for support, bug triage, user feedback, and controlled rollout conditions |
Vendor interviews should expose weak thinking fast. Broad questions produce rehearsed answers. Ask for specifics that reveal whether the team has done this work before.
What data in our MVP counts as personal health information, and where will each category live?
Which provincial rules could affect hosting, access, or consent if we launch in Canada first?
What artefacts do you produce during discovery? Architecture diagram, threat model, data flow map, backlog, or all of them?
Who makes security and privacy decisions on the project, and how are those decisions documented?
How would you design the MVP so later FHIR R4 or HL7 work does not force a rebuild?
How do you test permissions, audit trails, consent withdrawal, and edge cases around user access?
What part of our requested scope would you cut first, and why?
Strong vendors answer directly. Weak vendors stay vague, hide behind jargon, or promise that everything can be added later.
I would treat these red flags seriously:
A low quote with little detail: That usually means the proposal excludes security, compliance setup, documentation, or post-pilot fixes.
A HIPAA-only mindset: If Canada is part of your launch plan, a US-first compliance frame is incomplete from day one.
No clear discovery phase: That leads to avoidable rework, especially when sensitive data flows were never mapped properly.
No named security owner: Security by committee usually means security by neglect.
Pressure to build a broad platform early: Good partners protect your pilot by cutting scope.
No opinion on deployment or support: Shipping code is not the same as launching a HealthTech product safely.
The delivery model matters too. Early-stage founders usually do better with a specialist partner or a hybrid setup than with a rushed in-house build. You need category knowledge, speed, and clean decision-making. Permanent headcount can wait until the product has survived real pilot conditions and you know what capabilities belong inside the company.
Choose the team that challenges your assumptions, documents the invisible work, and designs for the market you are entering. In North America, that often means building with Canadian privacy requirements in mind first, then extending toward US expectations, not the other way around.
Hire the partner who asks harder questions before kickoff. That is usually the team protecting you from expensive mistakes.
Final Checklist and HealthTech Founder FAQs
A founder signs the proposal, starts design, and only then learns the pilot hospital wants Canadian data residency, role-based access logs, and a privacy review before a single user goes live. That mistake is avoidable. Use this section as a final gate before you spend another dollar.
Founder checklist before development starts
Run through these questions and do not proceed until each one has a clear answer.
What problem are you fixing first?
Name one painful clinical or operational problem. If it feels broad, it is still too vague.
Who is the primary user?
Choose one. Patient, clinician, admin, care coordinator, or payer. Secondary users can wait.
Where does personal health information enter, move, and rest?
Write out the flow. In Canada, that affects architecture, hosting, contracts, and budget immediately.
Which laws apply at launch?
Start with PIPEDA and the provincial rules tied to your pilot location, then map any US requirements if cross-border use is part of the plan.
What is the smallest product that proves value?
Cut anything that does not support the first workflow.
What future integrations are likely?
You do not need to build them now, but your data model should not create cleanup work later.
What does consent look like in the product?
Decide how users grant it, withdraw it, and how your team records it.
How will access be controlled?
Define roles, permissions, and audit expectations before design begins.
What are the pilot rules?
Specify the users, setting, support path, escalation process, and success criteria.
FAQs founders ask too late
How early should I plan for FHIR or HL7?
Plan for it during discovery. Do not force full integration into version one unless the pilot depends on it. But if your data model ignores FHIR or HL7 realities, you will pay for that shortcut later with rework, fragile APIs, and messy mapping.
What's the difference between a U.S. BAA and Canadian contractual expectations?
A BAA is a HIPAA mechanism. It does not cover Canadian obligations by itself.
If you are launching in Canada, your contracts need to match PIPEDA and the provincial privacy rules tied to your care setting, data location, and service model. That usually means sharper language around custody, access, breach handling, subcontractors, retention, and cross-border processing. Ask counsel to draft for the jurisdiction you are entering, not the one your vendor knows best.
Should I launch with mobile and web together?
Only if the workflow demands both. Founders often add a second interface too early and burn budget on duplicated QA, design, and support. If clinicians use desktops and patients never need an app in the pilot, build web first and prove adoption there.
Can I use offshore or generalist developers for a healthtech MVP?
You can use them if a qualified healthtech lead owns the architecture, security decisions, and delivery process. Otherwise, expect delays and avoidable compliance gaps.
General product teams often underestimate Canadian privacy requirements because they frame the project as a standard SaaS build with HIPAA added later. That is the wrong order. For a Canada-first MVP, privacy design, data residency decisions, auditability, and provincial expectations shape the build from day one.
What should I have in hand before I approve development?
Five things. A scoped pilot workflow, a written data-flow map, a jurisdiction-specific compliance brief, a delivery plan with milestones, and a proposal that separates product work from security and compliance work. If a vendor cannot present that clearly, do not sign yet.
Cleffex Digital Ltd is one option to evaluate if you need a Canada-first view of compliance, architecture, and vendor fit. The right next step is a discovery conversation that defines jurisdiction, data handling, pilot scope, and decision points before development starts.







