



North American healthcare SaaS is projected to grow at a 25 to 30% CAGR and reach about $50 billion by 2028, according to this healthcare SaaS market analysis. That number matters, but not for the usual reason. It doesn't just signal demand. It signals that more founders, clinics, hospitals, and investors will compete in a market where engineering quality decides who scales cleanly, who stalls in procurement, and who gets discounted during diligence.
In healthcare, a weak product isn't just inconvenient. It creates security exposure, slows legal review, breaks clinical workflows, and raises questions about who actually owns the codebase. That last issue is often missed until a financing round, acquisition review, or enterprise deal uncovers it.
I've seen teams treat healthcare SaaS engineering services as a build shop. That's the wrong frame. The right frame is risk management through architecture, delivery discipline, and clear IP control. Compliance is part of that. Scalability is part of that. Valuation is part of that too.
The Digital Transformation of Healthcare
Healthcare software is no longer a side system sitting behind the front desk. It now shapes triage, scheduling, clinical communication, patient engagement, analytics, remote care, and care coordination. The organisations moving well in this environment aren't merely buying software. They're building platforms that can survive procurement scrutiny and operational reality.
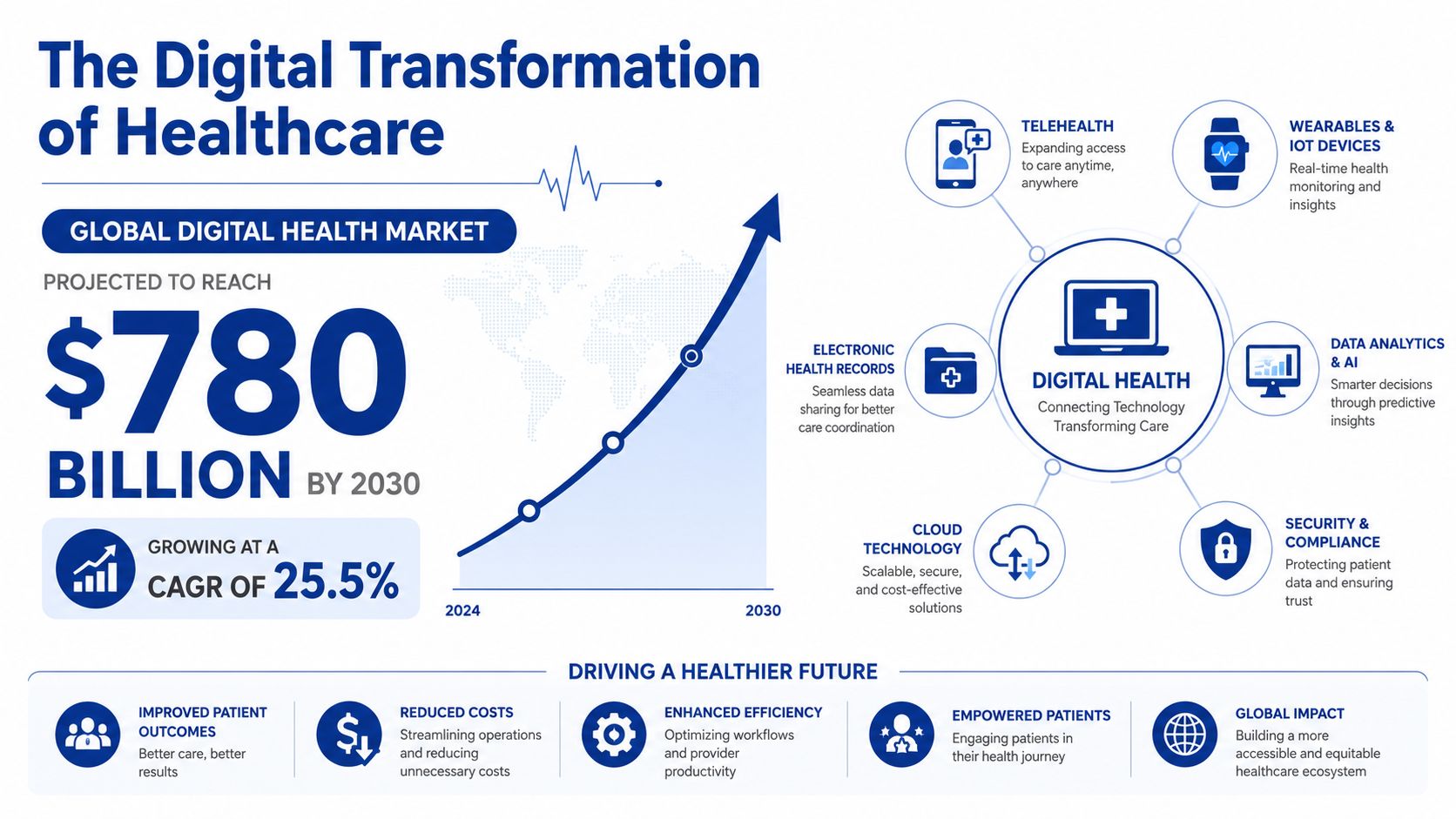
Three pressures are driving the shift in practical terms:
Remote care is now operational, not experimental: Teams need software that supports telemedicine, scheduling, secure communication, and reliable data exchange.
Data has to move across fragmented systems: If patient, provider, billing, and device data remain siloed, the product becomes a bottleneck instead of a service layer.
Personalisation depends on trustworthy inputs: Better recommendations, automation, and decision support only work when underlying records are structured and dependable. A useful reference on that front is this guide to AI solutions for healthcare data.
Many buyers still focus first on visible features. Patients can book. Clinicians can log in. Admins can send reminders. Those are table stakes. The engineering questions come next, usually when a deal is already under pressure. Can the system support regional privacy expectations? Can it integrate with existing hospital tools? Can it scale under uneven demand? Can it prove who accessed what and when?
Healthcare software usually fails in the seams. Integration seams, compliance seams, deployment seams, and ownership seams.
That's why healthcare SaaS engineering services matter. They bridge strategy and execution. They turn a concept into a cloud-native product with secure data handling, auditable controls, and a delivery model that doesn't collapse as customers become more demanding. If you're assessing how digital change affects software priorities across providers and healthtech firms, this overview of the digital transformation of healthcare is a useful companion read.
What Are Healthcare SaaS Engineering Services
General software development can produce a working app. Healthcare SaaS engineering services are different. They're the discipline of designing, building, integrating, securing, and maintaining healthcare software in a way that fits clinical operations and regulated data handling from day one.
A simple analogy helps. Building standard business software is like constructing an office building. Building healthcare SaaS is like building a hospital. Both need walls, power, and plumbing. Only one needs infection control, specialised airflow, emergency access, and strict operating procedures. The same logic applies to software.
The specialist roles you actually need
A credible healthcare engineering team usually combines several functions that generic developers often treat as secondary:
Solutions architecture for tenant design, platform boundaries, integration patterns, and data flow decisions.
Cloud engineering for resilient deployment on platforms such as AWS or Azure, including container orchestration and infrastructure automation.
Security engineering for encryption, secrets handling, key management, identity design, and auditability.
Compliance-aware delivery so technical decisions leave evidence that legal, privacy, and procurement teams can evaluate.
Integration engineering for EHR, EMR, pharmacy, lab, claims, scheduling, and patient-facing systems.
If one of those areas is weak, the product may still launch. It just won't travel well into due diligence, enterprise sales, or expansion.
What makes it different from ordinary SaaS work
Healthcare software handles more than user accounts and transactions. It has to reflect how care is delivered. That means understanding appointment logic, referral paths, consent flows, provider roles, patient communications, exceptions in clinical operations, and the practical consequences of downtime.
Here's where many projects go wrong:
| Generic software mindset | Healthcare SaaS mindset |
|---|---|
| Ship fast, harden later | Design for audit, privacy, and change control early |
| Integrate only when required | Plan for interoperability from the start |
| Store all data centrally by default | Design around residency, access boundaries, and sensitivity |
| Treat documentation as overhead | Treat architecture and controls as procurement assets |
Practical rule: If a vendor can describe screens but can't describe clinical workflow exceptions, they're not ready for healthcare work.
Healthcare SaaS engineering services also cover lifecycle questions that buyers underestimate. Who owns the source code? Who owns deployment scripts, infrastructure modules, and custom connectors? Who can maintain the platform if the relationship ends? In healthcare, those are not legal footnotes. They directly affect continuity, valuation, and exit options.
Core Capabilities You Must Demand
The fastest way to spot a weak healthcare vendor is to ask for specifics. Serious teams can explain architecture choices, control models, delivery workflows, and operational trade-offs in plain language. Thin teams hide behind buzzwords.
A baseline architecture in Canada should include auto-scaling infrastructure on AWS or Azure, Kubernetes for container orchestration, AES-256 encryption for data at rest, and TLS 1.3 for data in transit to satisfy provincial privacy obligations and demonstrate compliance, as outlined in this Canadian healthcare SaaS engineering guide. That baseline doesn't make a platform excellent. It makes it credible.
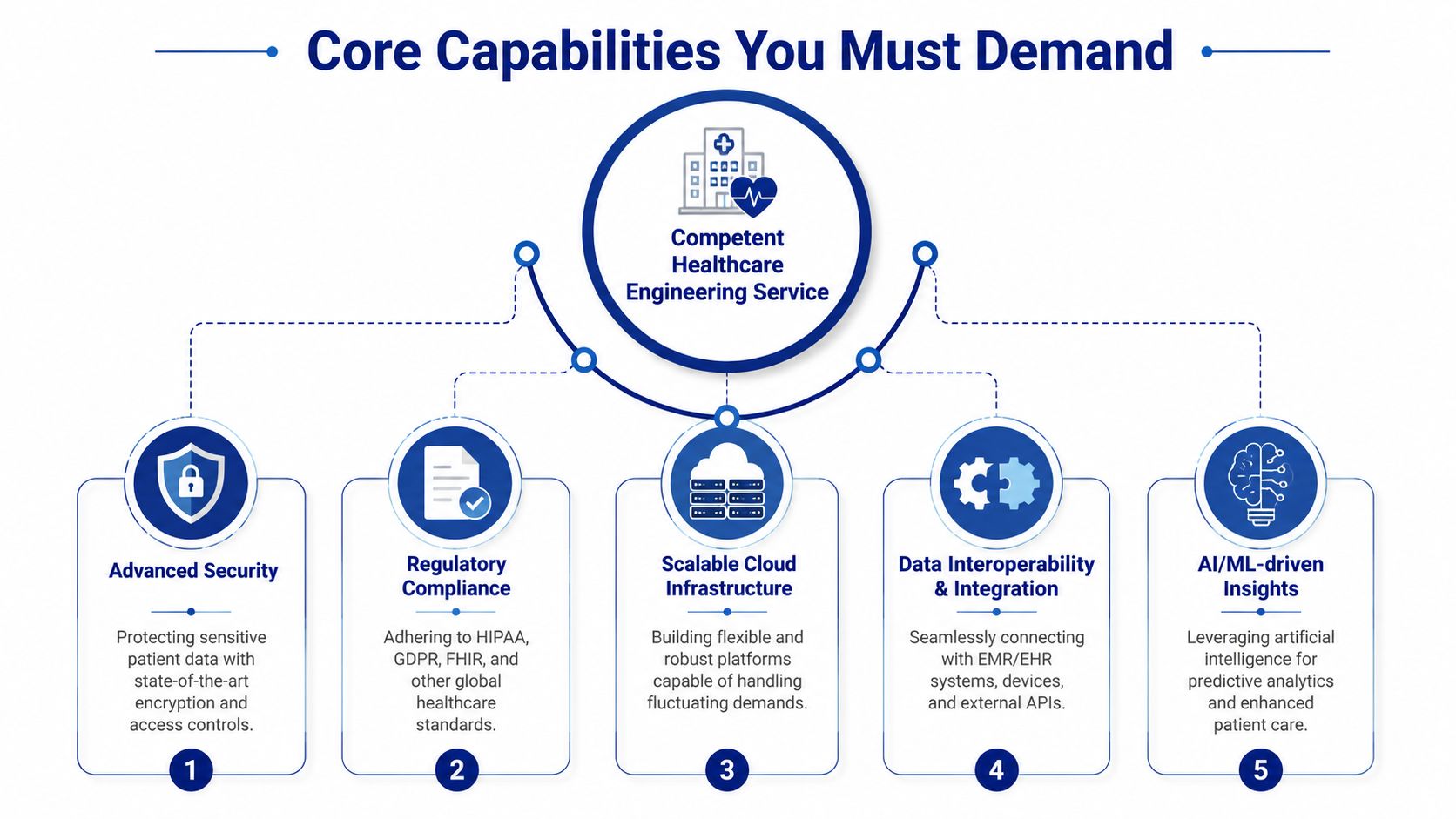
Security has to be structural
Healthcare buyers often hear “we use encryption” and move on. That isn't enough. You need to know where encryption is applied, how keys are managed, how access is segmented, and what evidence exists for audit review.
Strong security work usually includes:
Identity design: Role-based access is mapped to real operational roles, not generic admin and user buckets.
Audit logging: Access, data changes, and privileged actions are traceable.
Secrets management: Credentials aren't hardcoded into services or pipelines.
Environment separation: Development, staging, and production are isolated with controlled promotion paths.
If you want a practical external reference for evaluating controls and governance practices, this overview of modern cloud security practices is useful. For healthcare-specific concerns around PHI and system protection, this guide to data security in healthcare information systems adds good context.
Compliance must be visible in the build process
Compliance isn't a PDF created after launch. It's expressed in architecture, deployment, logging, retention, access approval, and documentation. Teams that only mention compliance in sales calls usually create rework later.
Look for evidence in places such as:
User stories and acceptance criteria that include privacy and audit needs.
Infrastructure templates that enforce standard controls across environments.
Release processes that document approvals, testing, and rollback capability.
Interoperability creates business leverage
A healthcare platform that can't exchange data cleanly becomes expensive to adopt. Interoperability is not just a technical standard. It's a sales enabler and a retention mechanism.
When a platform supports integration properly, it can:
fit into hospital procurement more easily
reduce manual staff work
support better patient journeys across systems
open opportunities for ecosystem partnerships
The technical side matters, but the business side matters more. FHIR and HL7 support are valuable because they reduce friction in real deployments.
Cloud resilience and DevSecOps separate mature teams from fragile ones
Healthcare traffic is uneven. A product may see calm baseline usage, then sharp spikes around campaigns, seasonal demand, or employer rollouts. Auto-scaling helps. So do queue-based workloads, stateless services, and well-defined failure boundaries.
A reliable vendor should be able to discuss this trade-off clearly:
| Capability | What works | What fails in practice |
|---|---|---|
| Deployment | Automated CI/CD with environment controls | Manual releases with undocumented fixes |
| Infrastructure | Reproducible templates and container orchestration | One-off server setup |
| Monitoring | Alerts tied to service health and user impact | Logs nobody reviews |
| Incident response | Runbooks, rollback plans, ownership | Slack improvisation at midnight |
Good healthcare engineering doesn't remove complexity. It contains it.
How to Structure Your Engineering Partnership
The way you buy healthcare SaaS engineering services matters almost as much as the team you choose. A strong vendor in the wrong engagement model can still create delay, confusion, and unnecessary cost.
Canada's product engineering services market generated USD 99.7 million in 2024 and is projected to reach USD 122.3 million by 2030 with a 3.6% CAGR from 2025 to 2030, according to this Canada product engineering services outlook. That same source notes that product development holds about 45% of market share, which aligns with what many healthcare buyers are already doing. They're not just buying staff hours. They're buying end-to-end product capability.
Three engagement models
Here's the practical comparison I use with clients.
| Model | Best fit | Main advantage | Main risk |
|---|---|---|---|
| Full outsourcing | Non-technical founders or lean internal teams | Fastest path to a managed build | Lower day-to-day technical control |
| Team augmentation | Existing product teams with specific gaps | Keeps internal ownership strong | Requires strong client-side management |
| End-to-end product development | New platform builds or major rebuilds | Aligned architecture, delivery, and lifecycle planning | Needs clear governance and decision rights |
How to choose without guessing
Pick based on your internal operating reality, not your aspiration.
Choose full outsourcing if your team doesn't have architecture, DevOps, compliance, and product delivery capacity in-house. This works when speed and completeness matter more than building an internal engineering department immediately.
Choose team augmentation if you already have strong product leadership and need targeted help. Typical gaps include cloud security, interoperability, DevSecOps, or senior backend engineering.
Choose end-to-end product development if you're creating a platform, not just shipping features. This model works well when you need architecture, UX, development, testing, compliance-aware delivery, and post-launch support tied together.
The hidden selection criterion
Most buyers focus on cost control. Fair enough. But the key differentiator is decision ownership.
If your internal team can set architecture, approve changes, manage backlog priorities, and review technical debt, augmentation can work well. If not, you need a partner who can own those responsibilities with discipline and documentation.
A weak partnership structure usually looks like this:
nobody owns architecture decisions
sprint velocity is discussed, but risk isn't
compliance questions go to legal after engineering choices are already locked in
release responsibility is split so widely that no one can answer for outcomes
That's why the most successful healthcare engagements define delivery governance early. Who approves technical standards? Who owns infrastructure? Who signs off on integrations? Who controls production access? Those answers matter more than the daily rate.
Selecting Your Healthcare SaaS Engineering Vendor
Vendor selection in healthcare should be treated like investment diligence. Procurement teams often compare hourly rates, team size, and slide decks. Investors and enterprise buyers care about something deeper. They want to know whether the product is built on engineering assets that can be trusted, transferred, scaled, and defended.
One issue deserves more attention than it gets: code risk. According to this Canada healthcare SaaS market outlook, Canadian healthcare SaaS revenue is projected to grow while investors increasingly ignore the code powering platforms, creating a valuation gap for startups that haven't addressed engineering due diligence. In practice, that means a startup can have demand, pilots, and a compelling story, yet still lose their advantage if buyers or investors find poor code quality, unclear ownership, or operational fragility.
What code risk actually means
Code risk isn't just buggy software. It includes several business-critical failures:
Unclear IP ownership: Contractors, subcontractors, or agencies may have created core components without clean assignment terms
Undocumented architecture: Key workflows exist only in developers' heads
Dependency fragility: Vital integrations or services rely on ad hoc implementations no one can safely modify
Security debt: Known shortcuts remain in production because deadlines won
Delivery concentration: One or two individuals effectively control the platform
None of those problems shows up on a polished demo.
Questions that reveal the real vendor
Ask direct questions and insist on concrete answers.
Who owns the source code, infrastructure code, and integration connectors when the engagement ends?
How do you document architectural decisions and handover assets?
What does your release pipeline enforce before production deployment?
How do you separate client-specific customisation from core platform code?
How do you handle privileged access, audit logging, and incident response?
What happens if we replace your team in twelve months?
A reliable vendor won't be offended by these questions. They'll be ready for them.
Evaluate for long-term transferability
Many healthcare products start with speed as the priority. That's understandable. But if the build model creates dependency on one vendor's tribal knowledge, the asset becomes harder to finance and harder to sell.
Use this quick lens during due diligence:
| Due diligence area | Healthy signal | Warning sign |
|---|---|---|
| IP and contracts | Clear assignment and repository ownership | Ambiguous subcontractor terms |
| Architecture | Decision records and system diagrams | “We can explain it live” |
| Delivery process | Repeatable, auditable releases | Manual deployment by a few people |
| Clinical fit | Workflow understanding and exception handling | Generic SaaS thinking |
| Exit readiness | Handover plan exists | No transition model |
If you can't transfer the system cleanly, you don't fully own the asset.
One practical option in the market is Cleffex Digital Ltd, which provides healthcare product engineering and integration services for secure, compliant platforms in Canada. What matters more than the vendor name, though, is whether any partner can prove disciplined engineering, clean ownership, and operational maturity under scrutiny.
Real-World Architectures and Case Studies
A telemedicine product sounds straightforward until you map the moving parts. Patients need a web or mobile interface. Clinicians need scheduling, records access, communication tools, and role-based permissions. Admins need reporting, auditability, and integrations. External systems may include pharmacies, labs, identity providers, and payment workflows.
This kind of architecture is common.
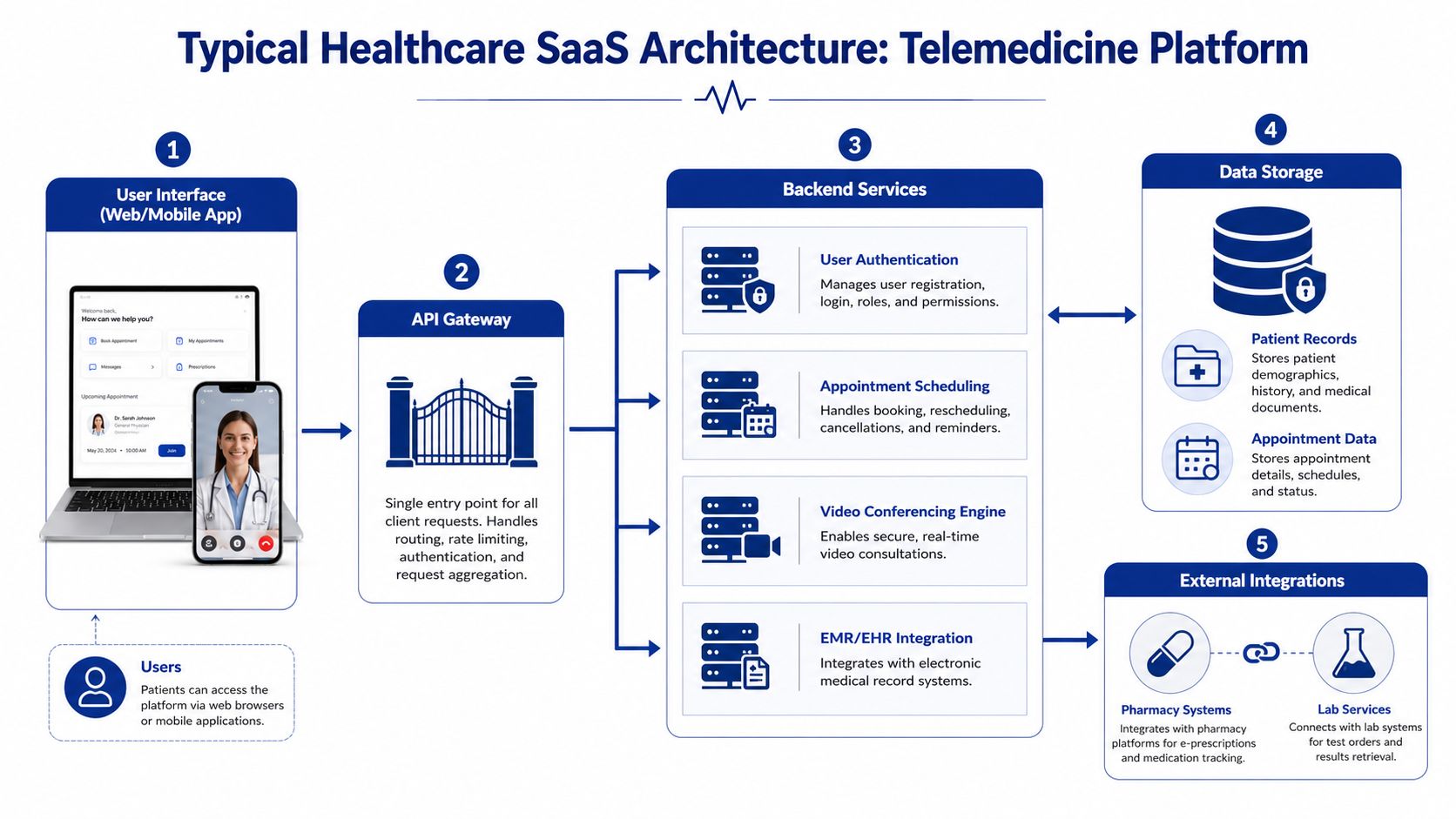
A practical architecture pattern
For telemedicine platforms, I generally favour a modular setup with clear service boundaries:
User interface layer for patient and clinician apps
API gateway for routing, authentication enforcement, and rate handling
Backend services for appointment scheduling, user management, notifications, and consultation workflows
Video service integration isolated from core clinical logic
Data layer separated by sensitivity and access patterns
External integration services for EHR, pharmacy, lab, or claims connectivity
Audit and observability services running across the stack
That pattern helps with scale, but its real value is operational containment. If video performance degrades, it shouldn't compromise scheduling or patient records. If a lab integration fails, it should queue and retry without corrupting core workflows.
For buyers thinking beyond a simple app build, this overview of enterprise healthtech platform development is worth reviewing because it shows how platform decisions shape growth and governance.
The enterprise virtual care trade-off
One of the hardest real-world design problems in Canada is the tension between enterprise virtual care for employers and the sustainability of the public healthcare system. This analysis of enterprise virtual care and public system implications highlights the architectural trade-offs around data sovereignty and resource erosion.
A realistic case looks like this.
An employer-sponsored virtual care platform wants fast onboarding, broad availability, and strong employee experience. That pushes teams toward centralised services, streamlined access, and aggressive automation. Public system realities pull in another direction. Data may need stronger sovereignty controls. Integration choices may need to respect provincial expectations. Care pathways must avoid fragmenting records or creating a parallel channel that weakens continuity.
What worked and what didn't
What works in these situations is deliberate architectural separation.
Separate employer administration from clinical data domains: HR-facing reporting should never sit too close to patient-level records.
Design data residency controls early: Retrofitting residency logic later usually creates painful migration work.
Create explicit integration boundaries: Enterprise convenience features shouldn't bypass public-system record flows.
Treat consent and access context as product features: They are not back-office settings.
What doesn't work is pretending a standard B2B SaaS pattern can be lightly adapted for healthcare. That usually produces confused identity models, mixed data domains, and procurement friction the first time a serious customer reviews the system.
Architecture decisions in healthcare often carry policy consequences, not just technical ones.
Your Buyer's Checklist for Success
A good selection process should leave you with evidence, not impressions. Use the checklist below when evaluating healthcare SaaS engineering services. If a vendor can't answer these points clearly, keep looking.
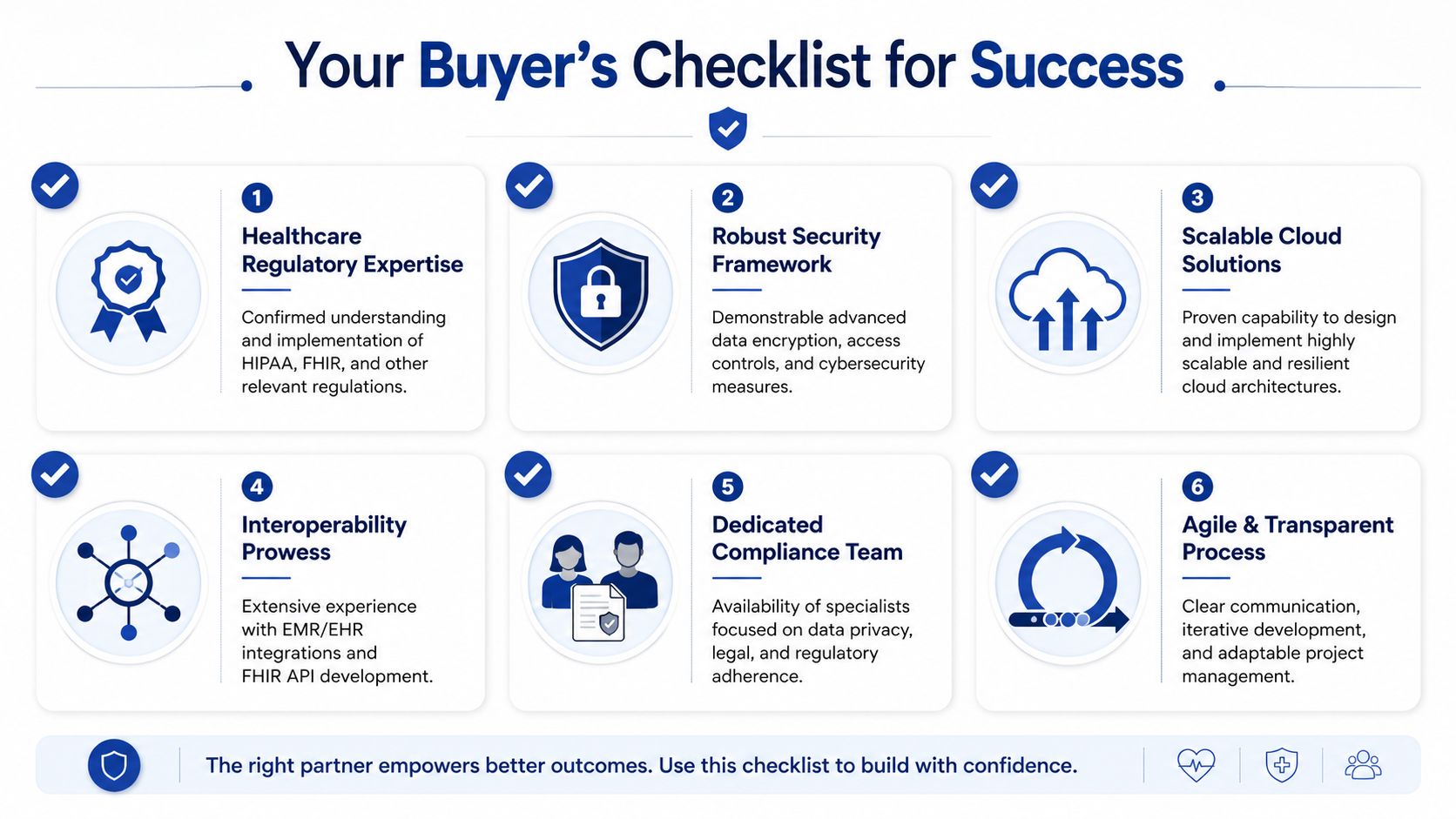
Technical due diligence
Request architecture artefacts: Ask for sample system diagrams, deployment patterns, and decision records.
Review release discipline: Confirm there's a real CI/CD process, rollback plan, and environment separation.
Check interoperability depth: Ask how the team approaches FHIR, HL7, and external healthcare integrations.
Test operational maturity: Ask who handles incidents, what gets logged, and how service health is monitored.
Compliance and security verification
Ask for control evidence: You want concrete examples of access control, audit logging, and encryption implementation.
Verify privacy-aware design: Make sure sensitive data handling is reflected in architecture, not just policy documents.
Examine access governance: Understand how privileged accounts, production permissions, and support access are managed.
Partnership and strategic fit
Clarify IP ownership in writing: Include source code, infrastructure code, documentation, and custom connectors.
Define handover expectations early: If the relationship ends, transition shouldn't become a crisis.
Match the engagement model to your team: A model that looks efficient on paper can fail if you lack internal oversight.
Assess clinical understanding: Vendors should understand workflow exceptions, not just user interface requirements.
Commercial and valuation protection
Probe for code risk: Ask what would stand up in investor, acquirer, or enterprise technical diligence.
Avoid key-person dependency: Make sure knowledge is distributed and documented.
Check scalability assumptions: Don't accept vague claims about growth readiness. Ask how the architecture supports real expansion.
The best buyers don't just ask whether a vendor can build. They ask whether the resulting software will remain secure, transferable, and investable.
Frequently Asked Questions
How long does it take to build an MVP for a healthcare SaaS product?
It depends on scope, integration depth, and compliance requirements. A basic workflow product with narrow functionality moves much faster than a platform that includes telemedicine, EHR connectivity, patient messaging, and multi-role permissions. The useful question isn't “how fast can you code it?” It's “what can we launch without creating architectural debt we'll regret in procurement?”
What usually drives cost the most?
Complexity drives cost more than feature count alone. Integrations, security controls, auditability, identity design, data handling rules, and deployment requirements all affect effort. Teams also underestimate the cost of fixing a weak first version. Rebuilds are expensive because they happen while the business is already trying to sell and support the product.
I'm a non-technical founder. What should I do first?
Start with three things: define the workflow problem, define the users, and define what data the product must handle. Then work with a senior architect or product engineering partner to shape an initial architecture and delivery plan. Don't begin with a freelance build brief full of screens and no system design.
How do we manage the vendor after launch?
Treat post-launch as an operating model, not a support retainer. You need release governance, security review, backlog ownership, incident handling, and clear rules for production access. Good partnerships become easier after launch because roles are clearer and the system is documented.
Do we really need to care about compliance so early?
Yes. Early doesn't mean doing every formal exercise on day one. It means making architecture choices that won't trap you later. If you want a plain-language overview of downstream exposure, this explainer on HIPAA compliance penalties is a useful reminder of why reactive compliance is costly.
What's the most overlooked issue in healthcare SaaS engineering services?
Ownership. Not just legal ownership of the company, but ownership of the code, infrastructure, deployment process, and knowledge. Products lose value when those assets are fragmented, undocumented, or dependent on one outside team.
If you're planning a healthcare platform, modernising an existing product, or assessing code risk before a funding or procurement milestone, Cleffex Digital Ltd can help you evaluate the architecture, delivery model, security posture, and ownership structure needed to build a secure, compliant, and investment-ready healthcare SaaS product.







