



A hospital CIO rarely has a data shortage. The problem is that the data needed for one decision usually lives in five places. A clinician opens the EHR for the patient chart, checks a separate lab portal for results, waits on imaging from PACS, asks finance for claims context, and still doesn't have a clean picture of what happened across the patient journey.
That friction shows up everywhere. Bed management teams work from delayed operational reports. Researchers spend more time reconciling fields than testing hypotheses. Security teams tighten access because broad sharing feels risky, which often pushes staff back to manual workarounds. The organisation ends up with plenty of data and very little shared truth.
A healthcare data fabric addresses that operational gap. It doesn't replace every existing system. It connects them, standardises how data is understood, and applies governance where access happens. For hospital leaders, that matters more than another storage platform. The architecture only creates value when clinicians, analysts, and administrators can use the right data quickly, without creating compliance problems.
From Data Chaos to Connected Care
A common hospital morning starts with a simple question that should have a simple answer: what does this patient need right now? Yet the answer often sits across admissions, lab systems, imaging, referrals, claims, and back-office applications that were never designed to work as one.
Clinicians feel it first. They don't describe the problem as “interoperability debt”. They describe it as repeated logins, duplicate data entry, and incomplete context during care decisions. Administrators see a different symptom. Reporting requests take too long because each request becomes a small integration project.
What the chaos looks like on the ground
In practical terms, disconnected systems create three kinds of drag:
Clinical drag: Teams make decisions with partial records because encounter history, medications, imaging, and social context aren't assembled in one usable view.
Operational drag: Reporting teams pull from siloed systems, clean data by hand, and still argue over which report is correct.
Strategic drag: AI, analytics, and population health programmes stall because the underlying data estate isn't organised enough to trust.
That's why data fabric is getting serious attention. The global data fabric market was valued at $2.1 billion in 2022 and is projected to reach approximately $8.9 billion by 2032, with a 15.54% CAGR from 2023 to 2032. In Canada, the related healthcare data collection and labelling market was USD 33.9 million in 2022 and is projected to reach USD 246.7 million by 2030, which signals growing demand for structured, interoperable health data in Canadian environments.
A useful way to think about a healthcare data fabric is this: it acts like a universal translator for health data. It doesn't force every source system into one giant replacement programme. It creates a connected layer that can interpret, organise, and govern information across those systems.
Broad access isn't the goal. Reliable, context-aware access is.
For teams also connecting clinical systems with devices and operational technology, Sheridan Technologies' guide is a practical companion because it highlights how integration pressure now extends beyond core hospital applications. The same pressure shows up in modern connected healthcare platforms, where patient experience depends on systems exchanging usable data rather than just messages.
Why this matters to a CIO now
The mistake is to treat data fabric as a technical fashion. It's not. It's a response to a hospital operating model that has outgrown point integrations and static reporting pipelines.
What changes with a healthcare data fabric is not just connectivity. The organisation gets a way to move from fragmented records to connected care, without pretending legacy systems will disappear any time soon.
Unlocking Strategic Value with a Data Fabric
For a CIO, the business case has to go beyond architecture diagrams. A healthcare data fabric is worth pursuing when it improves care delivery, reduces operational friction, and creates a foundation the organisation can keep building on.

Interoperability that means more than message exchange
Many hospitals already exchange data. That doesn't mean they've achieved interoperability in a useful sense. One system can send a record, and another can receive it, yet teams still spend hours reconciling terminology, patient identity, encounter context, and missing fields.
A healthcare data fabric improves this by creating a shared semantic layer over distributed systems. That means the organisation doesn't just move data. It understands what the data means in context. For clinical leadership, that's the difference between another interface and a usable patient view.
Better care decisions from a fuller patient picture
The strategic value becomes obvious at the point of care. When clinical, claims, imaging, and operational data can be assembled into a coherent whole, teams can act with more confidence. Discharge planning gets stronger when follow-up information is visible. Care coordination improves when referrals and prior interactions aren't hidden in separate systems.
This isn't about giving everyone everything. It's about giving each role the data needed for the decision in front of them.
Practical rule: If a clinician still has to ask three departments for a complete patient story, the architecture hasn't solved the problem.
Operational excellence without endless manual reconciliation
Most healthcare organisations understate the cost of data handling work. Not storage cost alone. Human cost. Analysts validating extracts. Interface teams remapping fields after source changes. Clinical operations waiting for reports built on brittle pipelines.
A data fabric reduces that burden by standardising how data is discovered, transformed, and delivered. That doesn't remove data engineering work, but it shifts effort away from repeated custom fixes and towards reusable services.
A platform for analytics and AI that won't collapse under scale
Hospitals want to use AI for clinical operations, risk identification, and service planning. Many can't move past pilot mode because the underlying data remains inconsistent, poorly governed, or inaccessible outside a narrow team.
A healthcare data fabric creates the conditions for production-grade analytics. The value is not that AI becomes possible in theory. The value is that data can be prepared and governed consistently enough for AI initiatives to move from isolated experiments to repeatable operational tools.
For leadership, that's the core argument. This isn't an IT side project. It's a business capability that supports care quality, operating efficiency, and long-term digital resilience.
The Architectural Blueprint of a Data Fabric
The cleanest way to explain a healthcare data fabric is to think of it as the organisation's digital nervous system. Source systems remain where they are, but the fabric connects them, interprets signals between them, and controls how information flows to the people and applications that need it.
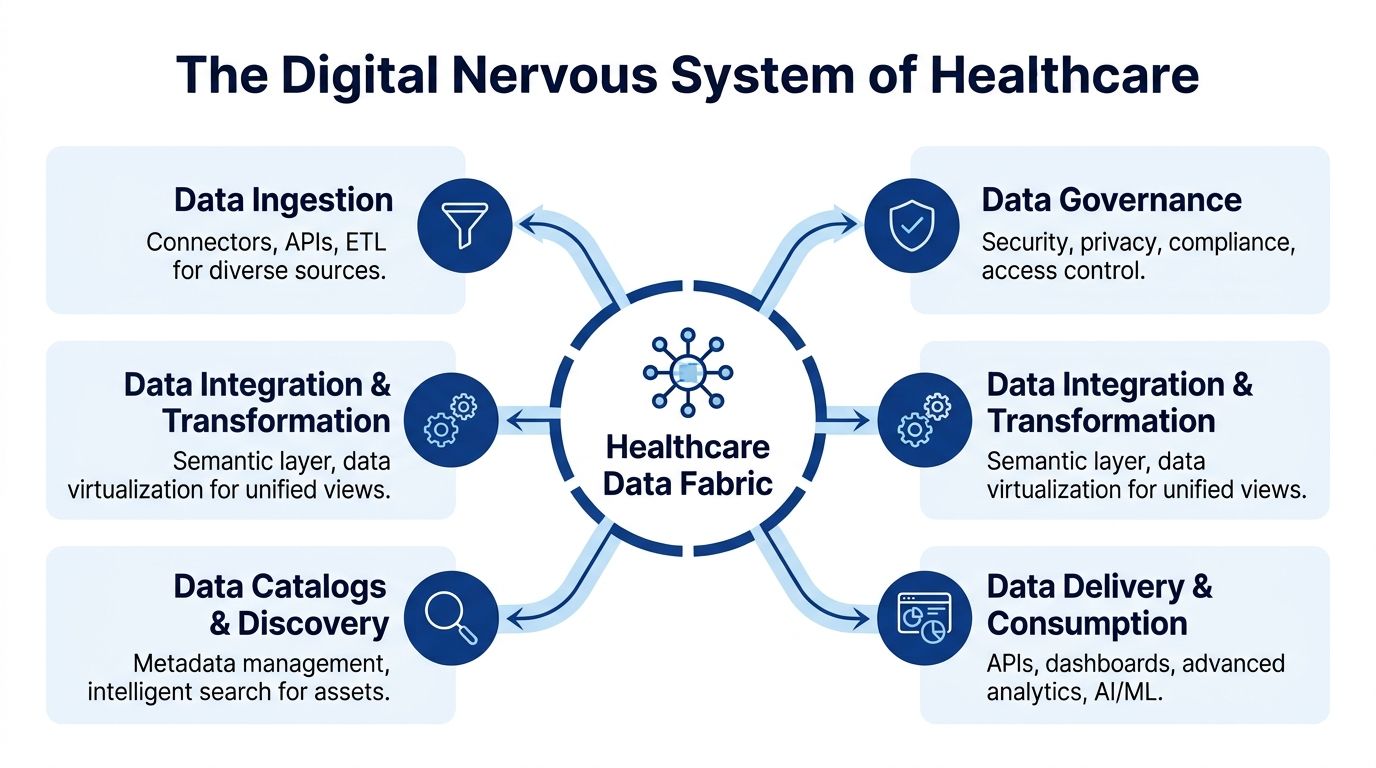
The components that matter
A working architecture usually includes several layers, each with a distinct job:
Data ingestion and connectors: These connect to EHRs, PACS, claims systems, laboratory platforms, DICOM repositories, and operational applications through APIs, event streams, batch pipelines, and existing interfaces.
Metadata and catalogue services: These tell teams what data exists, where it came from, who owns it, and how it should be used.
Semantic integration layer: Enables the organisation to map raw source data into shared concepts and business meaning.
Orchestration and transformation services: These automate movement, standardisation, enrichment, and delivery.
Governance and security controls: These enforce policies for access, quality, lineage, privacy, and auditability.
The semantic layer is the difference-maker. Without it, the architecture becomes a better plumbing system but not a better operating model.
Why HL7 FHIR matters in practice
Healthcare data fabric architecture works best when it uses open healthcare standards rather than inventing another proprietary model. Smile Digital Health's explanation of healthcare data fabric captures the key idea well: standards like HL7 FHIR let the fabric “wrap around” existing EHRs, ingest and clean trapped data, and create a unified information framework that supports semantic interoperability through native knowledge graphs.
That matters because most hospitals can't rip out core systems. They need an approach that works with the estate they already have. If your team is evaluating implementation patterns around FHIR integration services for healthcare interoperability, these services align with those patterns. They become one of the mechanisms that helps the fabric normalise and expose usable clinical data.
Data fabric versus warehouse thinking
A traditional warehouse can still play an important role. It just isn't enough on its own for healthcare's distributed, fast-changing data environment.
| Attribute | Healthcare Data Fabric | Traditional Data Warehouse / Lake |
|---|---|---|
| Primary design goal | Connect and govern data across distributed systems | Centralise data for storage and reporting |
| Fit for legacy healthcare estates | Designed to work around existing systems | Often depends on large-scale movement into a central platform |
| Semantic understanding | Strong focus on shared meaning and relationships | Often requires separate modelling work after ingestion |
| Operational responsiveness | Better suited to mixed real-time and near-real-time use | Commonly optimised for batch analytics |
| Governance model | Policy-driven access across sources and consumers | Frequently enforced after data lands in the platform |
| Time to initial use | Often faster when focused on high-value domains | Can slow down if the programme begins with full consolidation |
If your architecture requires every source system to be “fixed first”, the programme will stall before it delivers value.
The blueprint works when it stays federated where needed, standardised where possible, and governed everywhere.
Powering AI and Analytics in Healthcare
Once a healthcare data fabric is in place, data stops behaving like archived paperwork and starts behaving like an operational asset. That shift matters most in analytics and AI, where the limiting factor usually isn't model ambition. It's whether the organisation can deliver trusted, timely, context-rich data to the teams building and using those models.
The use cases that become realistic
Predictive analytics becomes more credible when risk signals can be assembled from multiple domains instead of one narrow clinical dataset. A patient's prior admissions, medication history, diagnostic results, care transitions, and administrative context can be analysed together rather than as disconnected snapshots. That gives clinical teams a stronger basis for intervention planning.
Population health work also improves. Chronic disease management, care gap identification, and service planning all depend on data consistency across sites, providers, and programmes. A data fabric doesn't solve those problems by itself, but it gives analysts a governed layer where cross-system patterns can be studied without rebuilding the pipeline every time a new source appears.
Operational AI needs governed data, not just more data
Some of the most immediate value comes from operational AI. Bed allocation, theatre utilisation, discharge coordination, staff scheduling, and supply planning all depend on data from systems that usually sit in separate silos. When those feeds are aligned under one governed architecture, hospitals can move from delayed reporting to decisions that support day-to-day operations.
Clinical trial recruitment is another strong example. Research teams often struggle to identify eligible cohorts because inclusion criteria span diagnoses, procedures, medications, imaging, and timeline events. A healthcare data fabric can reduce that search burden by exposing a more coherent view of patient populations across facilities.
What works and what usually fails
AI programmes succeed on top of a fabric when the organisation does three things well:
Starts with one or two high-friction decisions: Discharge risk, operating room flow, referral management, and similar use cases are often better starting points than “enterprise AI transformation”.
Treats data governance as part of model readiness: If access rules, lineage, and quality checks are weak, AI output won't be trusted.
Builds reusable data products: Each new use case shouldn't require a fresh round of interface archaeology.
What fails is familiar. Teams launch a model before they've stabilised data definitions. They centralise copies of sensitive data without role-aware controls. They optimise for dashboards, then discover that machine learning and operational workflows need very different delivery patterns.
For leaders assessing how analytics changes under modern tooling, Querio's AI BI for healthcare is useful reading because it frames AI-enabled business intelligence around actual healthcare decisions rather than generic reporting. That's the right lens. A healthcare data fabric isn't valuable because it stores more information. It's valuable because it helps organisations apply analytics and AI to real operational and clinical work without losing control of the data underneath.
Your Phased Implementation and Migration Plan
The fastest way to derail a healthcare data fabric initiative is to position it as an enterprise-wide replacement programme. That creates too much scope, too much fear, and not enough early proof. The better path is phased delivery with a narrow first target and hard governance from the start.

Phase one and two
Discovery and strategy should focus on one business problem that leadership already cares about. Good candidates include delayed clinical reporting, fragmented patient views, quality reporting bottlenecks, or poor data access for operational planning. At this stage, define the source systems, target users, access constraints, and success criteria.
Architectural design and pilot come next. Build the minimum viable fabric around a small set of systems and one governed use case. Don't start with every data domain. Start with enough scope to prove ingestion, semantic mapping, access control, lineage, and delivery.
Phase three and four
Phased rollout and migration means onboarding additional systems in an intentional order. Prioritise sources that expand value for the first use case or enable the next adjacent one. Keep old reporting or workflow paths running long enough to validate trust before switching users over.
Optimisation and scale are data platform patterns where many organisations finally realise whether they've built a platform or a one-off project. This phase should formalise operating ownership, improve metadata quality, harden data quality processes, and expand reusable services for analytics and application teams.
Pilot the governance model with the pilot use case. If you bolt governance on later, you'll redesign the platform under pressure.
Migration checklist
Use a checklist that covers technology, people, and process together:
Define the decision to improve: Pick a use case with visible operational pain and executive sponsorship.
Map the minimum source estate: Identify the EHR, claims, imaging, laboratory, and administrative systems required for that decision.
Choose build versus buy carefully: Buy commodity capabilities such as cataloguing, policy enforcement, and standard connectors when possible. Build only where workflows or data models are truly differentiating.
Assign data ownership: Name the clinical, operational, and technical owners for each domain before onboarding starts.
Design role-based access early: Don't wait until data has already been unified.
Run parallel validation: Compare new outputs with current reports and workflows until users trust the new layer.
Train actual users: Not just analysts. Include care coordinators, operations managers, compliance leads, and service desk teams.
Set an operating model: Decide who handles onboarding, policy changes, quality incidents, and semantic model maintenance.
A phased plan does something important politically as well as technically. It makes the programme governable. CIOs don't need another transformation initiative that promises everything and proves nothing. They need one that can show value, absorb legacy complexity, and expand without losing control.
Governing Data for Access and Compliance
This is the part most healthcare data fabric discussions underplay. Unifying data is hard. Governing unified data is harder. Once information becomes easier to reach, the central question changes from “can we connect it?” to “who should see what, when, and under which conditions?”
Correct access beats broad access
The key governance challenge is not broad access. It is correct access, fast enough for operations and controlled enough for compliance. Invene's discussion of Microsoft Fabric for healthcare payers points to the gap clearly: 50 to 90 per cent of healthcare data is siloed, yet most discussions stop at unification and fail to explain how policy-driven access control is implemented, especially in organisations dealing with legacy systems.
That gap matters in Canada. Hospitals and health networks often operate across regional constraints, mixed vendor estates, and different cloud patterns. A fabric that makes data more available can create a larger compliance problem if it doesn't enforce access at the policy layer.
What policy-driven control looks like
In practical terms, strong governance in a healthcare data fabric usually combines several mechanisms:
Role-based access control: A pharmacist, discharge planner, researcher, and finance analyst should not receive the same view of the same patient-related dataset.
Attribute-aware policies: Access can depend on department, care relationship, data sensitivity, location, and purpose of use.
Dynamic masking and tokenisation: Some users need partial visibility, not full record exposure.
Lineage and audit trails: Every important data element should be traceable back to source and transformation path.
Continuous data quality monitoring: Poor quality data is not only an analytics problem. It is a governance problem because bad data can drive bad decisions.
For organisations reviewing broader data security in healthcare information systems, the important point is that a fabric should enforce those controls consistently across data consumers, not leave each downstream application to improvise its own security model.
A secure healthcare data fabric doesn't ask users to be careful. It makes policy the default behaviour of the platform.
Compliance without operational paralysis
Hospital leaders often fear a trade-off between compliance and usability. In practice, weak governance creates both poor compliance and poor usability. Staff bypass cumbersome controls. Analysts build shadow datasets. Teams duplicate exports because the sanctioned path is too slow.
Good governance does the opposite. It gives the organisation a controlled way to open access where justified, while preserving auditability and privacy. That's what supports regulations such as HIPAA and PIPEDA in day-to-day operations. The answer isn't less access or more access. It's governed access that matches clinical, operational, and analytical purpose.
Measuring Success with KPIs and Case Studies
A healthcare data fabric should be judged the same way any major hospital platform is judged. Not by architectural elegance, but by operational and clinical outcomes. The strongest programmes define success in a way that both technology leaders and finance leaders can track.
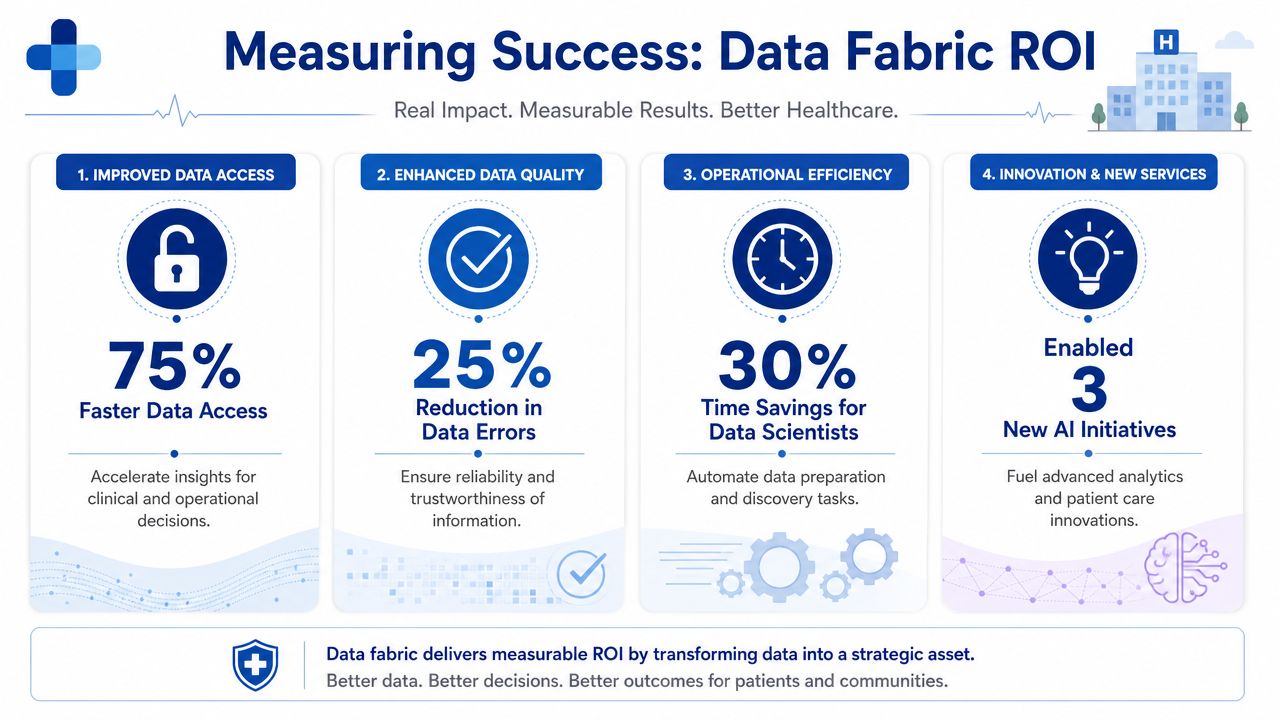
KPIs that actually matter
Useful measures usually fall into four groups:
Access and delivery metrics: Time required to provision a new data consumer, time needed to answer a recurring operational question, and stability of core pipelines.
Quality and trust metrics: Completeness, consistency, duplication resolution, and the volume of manual reconciliation still required after deployment.
Governance metrics: Audit readiness, policy coverage across datasets, and the reduction of uncontrolled extracts or shadow reporting.
Business and care metrics: Improvements tied to the initial use case, such as discharge efficiency, research cohort readiness, or reporting turnaround.
The right KPI set depends on the use case you start with. A population health initiative should not be measured the same way as a revenue cycle integration problem. But every programme should show whether the organisation is spending less effort assembling data and more effort using it.
A concrete proof point
One of the clearest quantified examples comes from California. In a setting where data warehousing costs can exceed $2.5M annually, a healthcare data fabric has been shown to reduce time-to-value by 50% and improve patient care outcomes by 25% through pre-built FHIR data pipelines and OMOP transformations, according to KMS Technology's healthcare data fabric case analysis.
That example is useful because it ties architecture to two executive concerns. First, speed. Second, outcome improvement. It also reinforces a practical lesson: pre-built standards-based pipelines can shorten the path to usable data when they are matched to the organisation's target operating model.
What a Canadian-style business case often looks like
A realistic Canadian scenario doesn't need invented numbers to be persuasive. Think of a multi-site clinic or hospital network trying to standardise referral visibility, quality reporting, and analytics access across a mixed legacy estate. The wins often appear as fewer hand-built extracts, faster onboarding of new reporting domains, stronger audit trails, and more consistent definitions between regional teams.
So, how are modern data platform patterns applied in adjacent operational environments? The specifics differ from acute care, but the underlying lesson is familiar: standardised data foundations create options that siloed systems don't.
The CIO's test is simple. If the new platform only centralises data, it's incomplete. If it improves governed access, accelerates delivery, and makes measurable operational outcomes easier to achieve, it's doing its job.
Cleffex Digital Ltd helps organisations design and build secure, interoperable software for complex industries, including healthcare. If you're evaluating how to modernise clinical data access, integrate legacy systems, or create a compliant foundation for analytics and AI, Cleffex Digital Ltd is worth contacting for a practical discussion.







