



A lot of Canadian healthcare leaders are in the same position right now. The EMR exists. Scheduling is digital. Lab, billing, and patient communication tools are in place. Yet staff still copy data between systems, clinicians still chase records, and every improvement request turns into an integration problem.
That's usually the moment when the search for a healthcare technology partner in Canada becomes serious. Not because the organisation wants another software vendor, but because it needs a partner that can work inside Canadian healthcare realities: provincial privacy rules, fragmented procurement, clinical workflow constraints, and the technical mess that sits between “system available” and “system useful”.
The right partner helps a hospital, clinic, or digital health team reduce friction without creating new risk. The wrong one delivers a polished demo, then struggles with workflow fit, privacy obligations, and integration depth once the project starts.
Why Choosing the Right Technology Partner Is Critical in 2026
By now, most Canadian providers aren't asking whether healthcare should be digital. They're dealing with a tougher question. Why does care still feel disconnected when so many systems are already in place?
The scale is clear. In 2024, 92% of Canadian healthcare providers had access to a digital health system, yet 78% still faced barriers to sharing patient information electronically, according to Statistics Canada's national digital health survey release. That gap is where many projects fail. The software exists, but the information flow, clinical fit, and operational design don't.
A hospital CIO usually sees this first in the form of small operational failures that add up:
Referral delays because clinical summaries don't move cleanly between systems.
Duplicate work occurs when staff re-enter patient information into portals, spreadsheets, or downstream applications.
Clinician frustration when a new tool adds steps instead of removing them.
Procurement fatigue occurs when vendors talk about innovation but avoid specifics on integration, support, and governance.
This is why a technology partnership matters more than a software purchase. You aren't just buying a product. You're choosing a team that will influence data movement, frontline workflow, compliance posture, and delivery risk.
Practical rule: If a partner can't explain how they'll reduce workflow friction in your actual care setting, they're not ready for Canadian healthcare delivery.
A useful way to frame the decision is this. Many vendors can build features. Fewer can operate as a true digital transformation partner for complex organisations where progress depends on integration, governance, change management, and long-term support.
What Works and What Does Not
What tends to work is narrow, operationally grounded planning. A partner starts with one care pathway, one user group, one data flow, and one decision-maker accountable for adoption.
What tends not to work is broad “platform modernisation” language without clear ownership. In Canadian healthcare, projects stall when nobody has mapped the clinical use case, the privacy boundaries, or the integration dependencies before procurement begins.
The Real Decision in Front of You
The question isn't whether to modernise. It's whether your organisation will choose a partner that understands how Canadian care environments function. That means provincial constraints, multi-stakeholder governance, and the fact that a technically successful deployment can still fail if staff don't trust it or if it doesn't fit the care process.
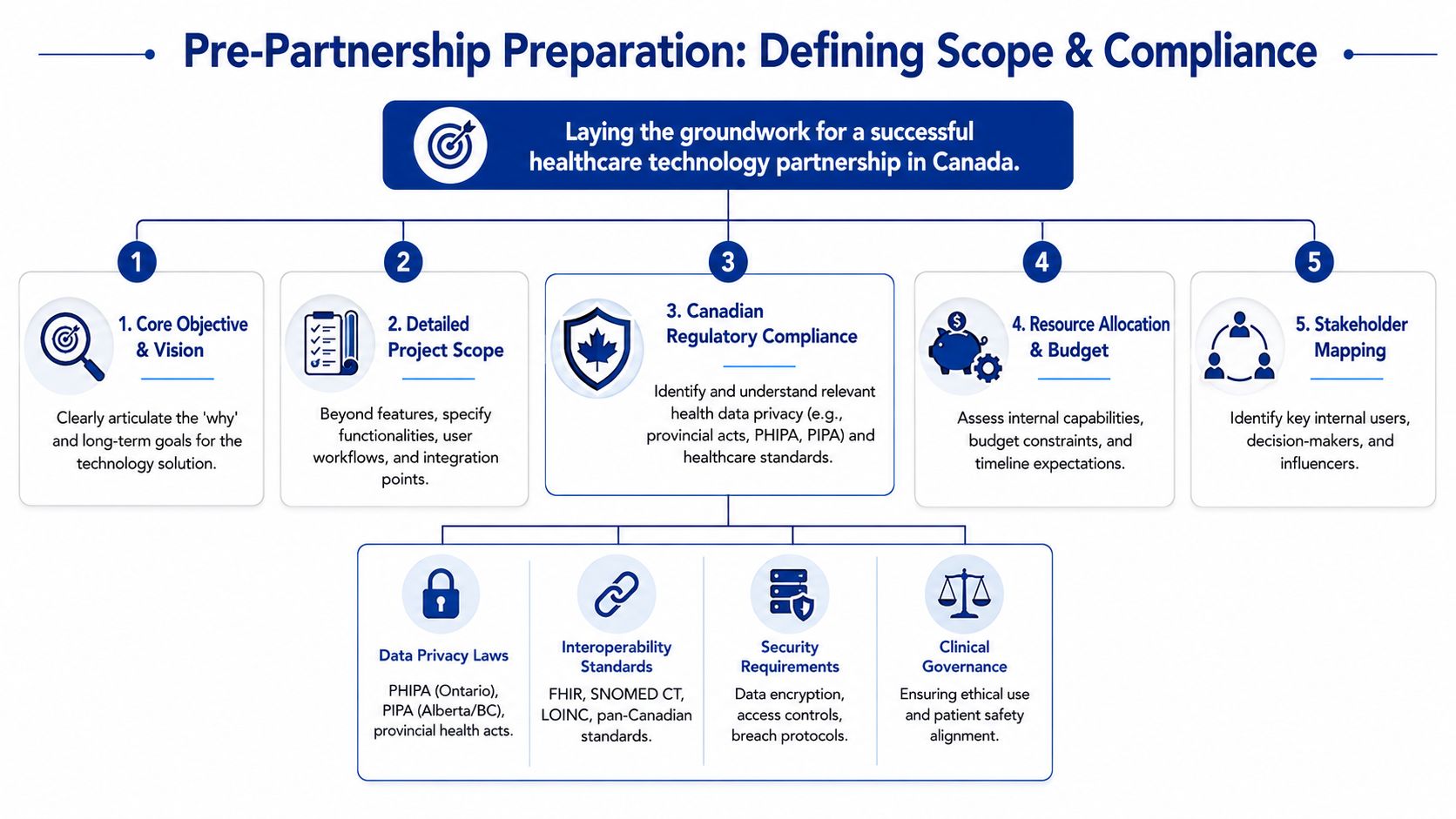
Define Your Project Scope and Canadian Compliance Needs
Before evaluating vendors, tighten your internal brief. Most failed partnerships don't start with bad intentions. They start with a vague scope.
Ontario Health's assessment model is a strong discipline to borrow from. Its workflow is to define the scope, evaluate the evidence, and make a recommendation, with PICO(TS) used to frame the problem in terms of population, intervention, comparator, outcome, time, and setting.
Start With the Care Problem, Not the Feature List
If your brief says “we need a patient platform” or “we need better interoperability”, it isn't ready. A stronger brief sounds more like this:
Population matters. Which patients or clinicians are affected?
Intervention must be specific. Are you adding a virtual triage layer, a referral connector, or a data-sharing workflow?
A comparator keeps the project honest. What current process are you replacing?
The outcome should be observable in operations or care delivery.
Setting matters in Canada because implementation conditions differ between hospitals, community clinics, and virtual care environments.
This level of detail immediately changes vendor conversations. It filters out generic responses and surfaces partners who can think clinically as well as technically.
Build Compliance Into the Scope From Day One
Canadian healthcare buyers often treat compliance as a review step near the end. That creates rework. Privacy, security, and data-handling rules need to be included in the first draft of the scope.
For most organisations, that means documenting:
Applicable privacy law, such as federal obligations and relevant provincial legislation, including frameworks like PHIPA or provincial private-sector privacy, rules where relevant
Data residency expectations if your organisation or funder requires data handling constraints
Access controls, including user roles, least-privilege design, and auditability
Breach and incident procedures with named responsibilities on both sides
Clinical governance for how the system affects safety, escalation, and accountability
A vendor response that skips straight to features and timelines, without engaging your privacy and governance questions, tells you a lot.
A practical internal exercise is to write the first version of your project brief as if legal, privacy, clinical operations, and IT all have to approve it together. That discipline exposes weak assumptions early.
Define What Your Team Can and Cannot Support
Hospitals and clinics often underestimate internal capacity constraints. Even a sound solution can fail if nobody owns data mapping, pilot design, clinician training, or post-launch issue triage.
Create a pre-partnership checklist that covers:
Decision ownership across IT, operations, privacy, and clinical leadership
Internal artefacts such as workflow maps, interface inventory, and policy requirements
Budget boundaries, including build, implementation, and support expectations
Operational readiness for testing, training, and adoption support
Procurement documents that reflect your real requirements, not recycled generic language
Teams that still depend on manual forms and loosely managed documentation often benefit from standardising the operational layer before a new system arrives. Resources like SheetMergy for clinic templates can help clinical and administrative teams clean up template sprawl so requirements are based on current reality, not fragmented paperwork.
If you're shaping a wider product or platform initiative, Cleffex's perspective on enterprise healthtech platform development is also relevant because it reflects the kind of architecture and delivery questions a serious partner should be able to answer.
How To Create Your Vendor Evaluation Checklist
Once your scope is solid, stop relying on sales calls and polished decks. Use a scoring model. It keeps the process fair, and it protects the organisation from choosing the vendor with the best presentation instead of the best operational fit.
A good checklist should test four things at once. Can the vendor work in Canadian healthcare? Can they integrate properly? Can they support adoption? Can they operate in a way your organisation can govern?
Vendor Evaluation Checklist
| Evaluation Criterion | What to Look For | Score (1-5) |
|---|---|---|
| Canadian healthcare experience | Relevant work with hospitals, clinics, health systems, or health startups in Canada. Clear understanding of provincial differences and healthcare procurement realities. | |
| Clinical workflow fit | Ability to discuss real user journeys for clinicians, administrators, and patients, not just features. | |
| Privacy and security maturity | Documented policies, clear role definitions, breach handling process, access control model, and secure development practices. | |
| Interoperability capability | Practical experience with healthcare data exchange, standards-based integration, API design, and EMR connection planning. | |
| Delivery governance | Named project roles, escalation paths, risk register approach, testing method, and change control discipline. | |
| Implementation support | Training plan, cutover support, issue triage, documentation quality, and post-launch service model. | |
| Equity and access approach | Concrete answers on accessibility, underserved users, language, usability, onboarding, and support design. | |
| Commercial clarity | Transparent pricing structure, assumptions, exclusions, and support terms. | |
| Reference quality | Verifiable client references or examples that speak to implementation quality, not just product capability. | |
| Working style and fit | Responsiveness, clarity, honesty about risks, and ability to collaborate with internal teams. |
Questions That Reveal Substance
Ask questions that force specifics. For example:
“Describe a healthcare integration you've delivered where workflow changed after testing. What changed and why?”
“Who on your side handles privacy design, security review, and integration architecture?”
“How do you deal with competing priorities between clinical leadership and IT?”
“What assumptions are you making about our internal team?”
“Which parts of implementation usually create delays?”
These questions matter because weak partners often answer with capability statements. Strong partners answer with delivery mechanics.
Don’t Skip Equity and Underserved Populations
This is one of the easiest areas for vendors to talk around. They'll often say their solution supports rural or underserved communities, then offer little detail on usability, onboarding, access barriers, or assisted support models.
That's a problem in Canada. Research on Ontario virtual urgent care found that underserved communities, including people with disabilities and visible minorities, can still face meaningful barriers to access, as discussed in this peer-reviewed study on virtual urgent care access barriers.
So ask direct questions:
Accessibility design. How does the product handle readability, assistive technologies, and low-friction navigation?
Digital access barriers. What happens when patients have low digital confidence or inconsistent connectivity?
Implementation equity. How will the rollout avoid privileging already well-served populations?
Support model. Is there a path for human assistance when self-service fails?
A partner who treats equity as a communications topic instead of an implementation issue will create problems later.
For procurement and finance teams, it also helps to apply classic supplier discipline. Controlling costs through IT vendor management is useful here because healthcare projects often drift when roles, service expectations, and change requests aren't tightly managed.
If you want a benchmark for what a technically grounded delivery partner should look like, review the public positioning of Cleffex Digital. The useful question isn't whether the website sounds polished. It's whether the partner can discuss architecture, compliance, integration, and support in enough detail to survive due diligence.
Mastering Interoperability and EMR Integration
In most Canadian healthcare projects, interoperability is where ambition meets reality. The organisation already has an EMR, sometimes several. It may also have lab systems, imaging platforms, patient portals, scheduling tools, billing workflows, and provincial reporting requirements. The challenge isn't adding one more application. It's making information move safely and usefully.
The national baseline is high, but the exchange layer is still thin. 93% of primary care physicians in Canada used EMRs in 2022, yet only 29% of physicians nationally shared patient clinical summaries electronically in the most recent 2024 survey. That tells you where to focus partner evaluation. Not on whether they can “work with EMRs”, but on whether they can deliver meaningful exchange.
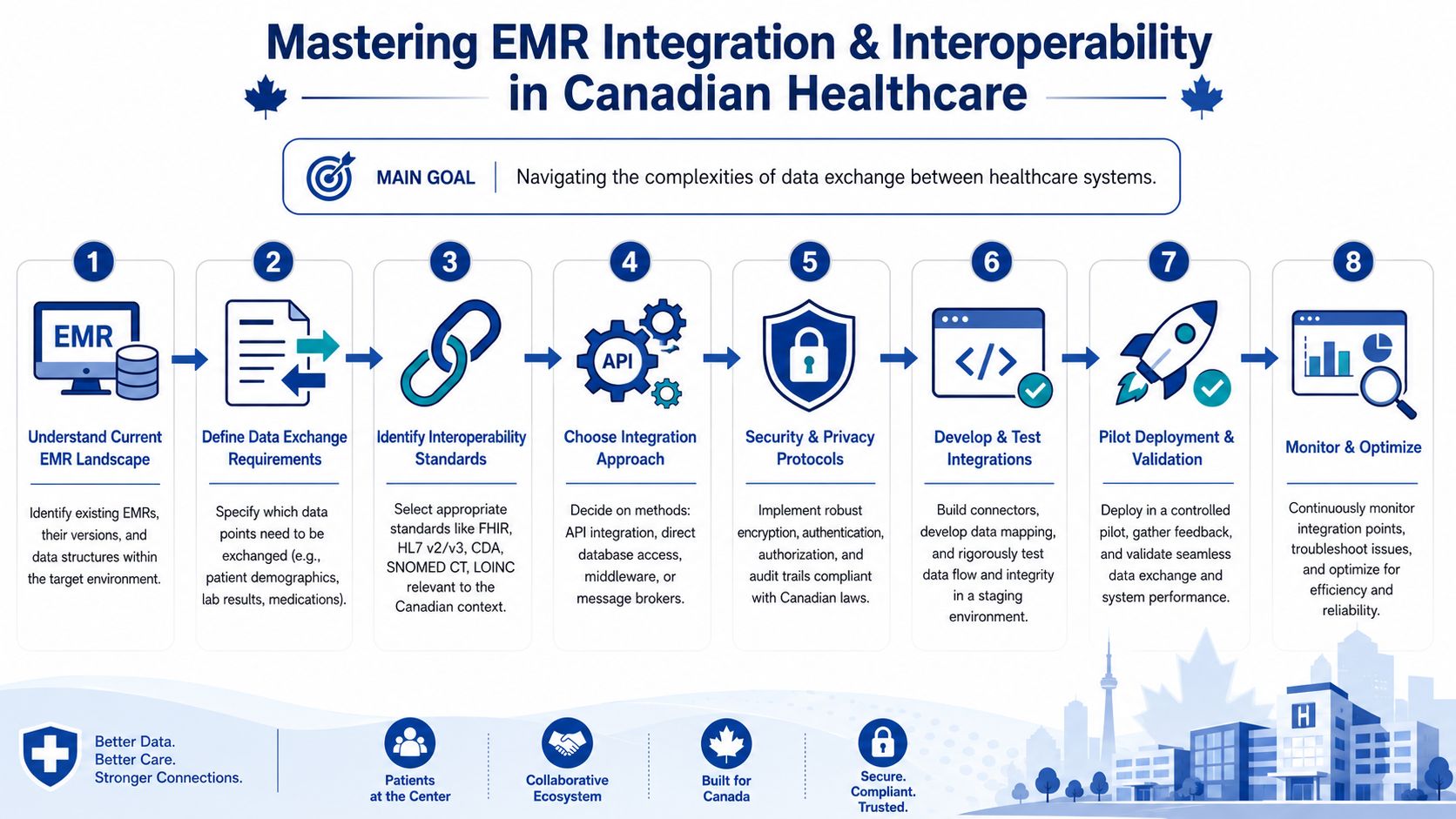
What Interoperability Actually Means in Practice
In a hospital or clinic setting, interoperability usually comes down to a short list of hard questions:
Which data elements need to move?
In what direction?
At what point in the workflow?
Under whose authority?
With what validation and audit trail?
That's where standards matter. FHIR, HL7 messaging, SNOMED CT, and LOINC aren't just technical terms. They shape how patient demographics, orders, results, medication information, and summaries are represented and exchanged.
A partner that understands this won't promise “full integration” in a discovery call. They'll ask for interface inventories, message examples, workflow maps, test environments, and exception handling rules.
Questions To Ask Your Partner
Use pointed language. Ask:
Describe your approach to integrating with existing EMRs rather than replacing them.
What standards do you commonly use for healthcare data exchange in Canada?
How do you handle data mapping, validation, and reconciliation when source systems disagree?
Have you integrated with provincial repositories, shared care environments, or multiple downstream systems?
How do you monitor failed messages, incomplete records, and audit events after go-live?
A specialist referral workflow is a useful example. A patient is seen in the hospital, then referred to a specialist using a virtual care tool. If the system can pull a current clinical summary, medication list, and referral context into the specialist workflow, staff avoid duplicate entry and clinicians make decisions with better context. If the partner only syncs demographics and leaves the rest to PDFs, email, or manual uploads, the “integration” is mostly cosmetic.
Strong integration work is boring in the right way. It is precise, tested, and visible in daily operations only because the staff stop noticing the friction.
For readers who want a simpler non-healthcare framing of integration pitfalls, this guide on data integration for SMBs is a helpful companion because many of the same issues apply: mismatched data, disconnected tools, and unclear ownership.
A more healthcare-specific view of these implementation questions is covered in Cleffex's article on EHR integration for healthcare providers, which is worth reading alongside your vendor assessment.
Structuring Pilots, Pricing, and Partnership Agreements
A smart healthcare buyer doesn't begin with a broad rollout. Start with a pilot that is small enough to control and meaningful enough to prove whether the partnership works.
That matters even more in the current market. Canadian health-tech investment became more selective in 2024, with venture funding falling 18% year over year to $700 million across 287 deals, according to the Canadian Health Tech Funding and Trends Report 2024. Buyers should read that signal carefully. The market is still active, but tolerance for vague ROI has dropped.

Design a Pilot That Answers One Business Question
A weak pilot tries to prove everything. A good one answers one strategic question clearly.
Examples include:
Can this workflow remove manual re-entry between two systems?
Can this tool improve handoff quality for one referral pathway?
Can this patient-facing workflow be adopted by a specific clinical team without adding support burden?
Set the pilot around one service line, one data exchange path, one operating team, and a limited time window. Define what counts as success before the build starts. Avoid success criteria like “positive feedback” alone. Include operational measures your own organisation can observe, such as completion reliability, turnaround consistency, or reduction in manual intervention.
Choose the Pricing Model That Matches Uncertainty
Different engagement models work for different project phases.
Fixed Price
Use this when the scope is stable and the interfaces are well understood. It gives budget clarity, but can become rigid when integration details change.
Time and Materials
Use this when discovery is still uncovering workflow or technical complexity. It's more flexible, but it demands stronger governance from your side.
Dedicated Team
Use this when the partnership is strategic and likely to expand across multiple releases. This model can work well if your organisation has product ownership maturity and wants continuity of domain knowledge.
The mistake is choosing the model for procurement convenience rather than project reality. In Canadian healthcare, integration unknowns often make pure fixed-price contracts fragile unless discovery has been done properly.
Contract Terms That Deserve Close Attention
The Statement of Work should do more than define tasks. It should reduce ambiguity.
Review these areas closely:
Scope boundaries that state what is included, excluded, and dependent on third parties
Data handling obligations covering access, storage, transfer, incident response, and audit support
IP ownership for custom code, configurations, documentation, and reusable components
Service levels for support response, defect handling, and severity classification
Acceptance criteria tied to tested outcomes, not informal sign-off
Change control with a documented method for handling new requirements
Exit provisions so the organisation can transition support or maintain continuity if the relationship ends
If the contract is vague on support, ownership, and change control, the pilot may succeed, but the long-term relationship will still become expensive and difficult.
Procurement teams often focus heavily on price, but in healthcare, that can be misleading. The cheaper proposal can cost more if it leaves internal staff to absorb testing, documentation, clinical configuration, and post-launch support.
Your Next Steps to a Successful Technology Partnership
Choosing a healthcare technology partner in Canada isn't a standard vendor selection exercise. It's a governance decision, a clinical operations decision, and a technical architecture decision at the same time.
The strongest process usually looks simple from the outside. Define the care problem tightly. Build compliance into the brief. Evaluate vendors with a scoring model instead of intuition. Treat interoperability as a delivery discipline, not a buzzword. Start with a pilot that proves value without exposing the whole organisation to avoidable risk. Then put the commercial terms in writing with enough precision that both sides know how success will be judged.
That approach protects more than the budget. It protects clinician time, patient trust, internal credibility, and your ability to scale once the first deployment goes live.
If your team is preparing for a first major partnership or trying to recover from a stalled one, the right next step is a structured discovery process with people who understand healthcare workflows, integration, and Canadian delivery constraints. The partner you choose should be able to speak clearly about those trade-offs before any code is written.
Frequently Asked Questions
| Question | Answer |
|---|---|
| What should a Canadian healthcare organisation own in the contract? | Own the business requirements, governance decisions, and any custom deliverables your organisation is paying to create, subject to negotiated terms. Clarify ownership of source code, configurations, interfaces, documentation, and reusable vendor components before work starts. |
| Is a software vendor the same as a healthcare technology partner? | Not always. A vendor may sell a product. A partner should also handle implementation planning, workflow alignment, risk management, support, and integration responsibilities in a way that fits your organisation. |
| Should we run a pilot before a full rollout? | Usually, yes. A pilot reduces risk and tests both the product and the working relationship. Keep it narrow enough to manage and specific enough to answer a meaningful operational question. |
| How do we evaluate privacy readiness when the delivery team is remote? | Ask where data will be accessed, who will have access, how permissions are managed, what audit records exist, and how incidents are escalated. Remote delivery isn't the core problem. Weak controls are. |
| What's the biggest red flag in a vendor proposal? | Generic language. If the proposal talks broadly about innovation but says little about workflows, interfaces, support boundaries, or compliance obligations, expect problems later. |
| How important is interoperability experience compared with product features? | In Canadian healthcare, it's often more important. Features are visible in demos. Integration quality determines whether staff can actually use the tool without adding friction. |
| How should hospitals handle stakeholder disagreement during selection? | Put the decision criteria in writing before final scoring. Clinical leaders, privacy, IT, procurement, and operations often value different things. A shared scorecard prevents late-stage conflict and makes trade-offs explicit. |
| What should we ask about post-launch support? | Ask who handles incidents, how severity is defined, what response expectations apply, how updates are governed, and whether training and documentation are included after go-live. |
If you're looking for a practical partner to help scope, integrate, and deliver healthcare technology in the Canadian market, Cleffex Digital Ltd works on secure software, healthtech integration, and healthcare product development with a delivery focus on compliance, workflow fit, and implementation support.







