



Patient engagement technology decisions now shape more than digital access. They affect intake flow, follow-up reliability, staff workload, and whether patients can participate in care without friction.
Many buyers still start in the wrong place. They compare portal features, reminder tools, telehealth modules, intake forms, and AI chat options, then move straight to EHR integration and privacy review. Those checks are necessary, but they do not tell a clinic director whether patients helped define the workflow, whether the tool reflects the needs of different patient groups, or whether it will reduce work instead of shifting it to staff and patients.
That design gap matters. A patient-facing system can meet procurement requirements and still fail in practice if older adults struggle with the interface, if language support is weak, if message timing creates confusion, or if AI-generated responses do not match clinical expectations. In my experience, adoption problems usually begin there, long before anyone blames the software vendor.
The stronger approach is layered. Clinics should involve patients in selection, workflow design, testing, and post-launch refinement, especially for AI-enabled tools that handle questions, triage simple requests, or support outreach. That is how organisations move past digital adoption and toward patient-centred systems that work in Canadian care settings.
It also changes the buying criteria. The right platform is not just the one with the longest feature list. It is the one your team can govern properly, measure clearly, and adapt with patient input over time, whether you are deploying in-house tools or working with outside solutions for healthcare support teams.
Why Patient Engagement Technology Is a Top Priority
Canadian healthcare research found that 77.9% of respondents saw patient engagement activities disrupted during the pandemic. For clinic leaders, that result matters less as a pandemic snapshot than as a warning. Many organisations added digital touchpoints quickly, but speed did not guarantee a better patient experience or better operations.
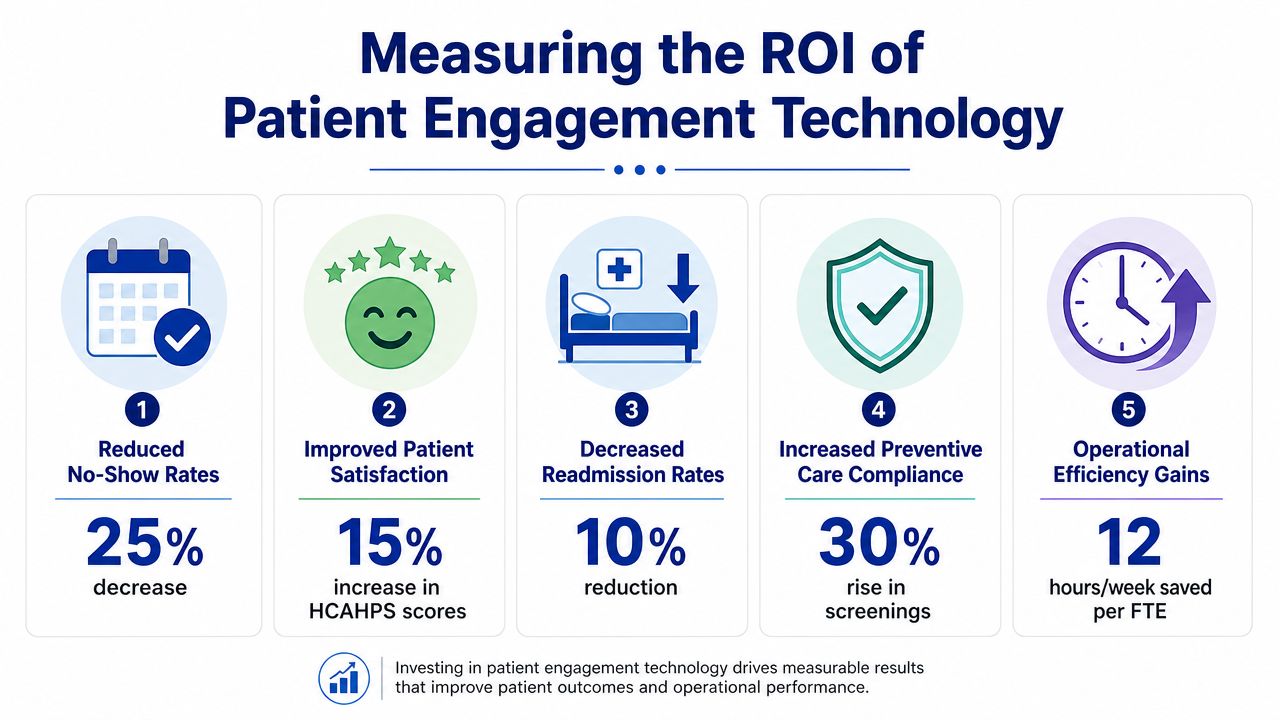
Patient engagement technology now affects three things every director is accountable for: access, staff workload, and revenue protection. A reminder system that cuts no-shows helps access. A portal that shifts routine questions away from phones helps staff capacity. A follow-up workflow that gets patients to complete the next care step protects downstream billings and reduces drop-off.
The primary priority, though, is not feature adoption. It is design discipline.
A clinic can buy messaging, intake, reminders, self-scheduling, and AI chat in one platform and still miss the point if patients were never involved in shaping how those tools work. That is one reason engagement programmes stall after procurement. The technology is live, but the workflows reflect internal assumptions instead of patient behaviour, language needs, trust concerns, or accessibility constraints.
I see this problem often with AI-enabled tools. Buyers ask whether the assistant can answer FAQs or route requests. They should also ask who reviewed the conversation flows, which patient groups tested them, how escalation works when the model is wrong, and whether the tool reduces phone volume without creating new review work for nurses. That is the difference between digital access and patient-centred design.
Practical rule: If a platform adds another inbox, another login, or another manual step for nurses, it is adding cost, not improving engagement.
For software buyers, procurement should focus on operating fit. That includes governance, workflow ownership, consent handling, language support, accessibility, escalation rules, and reporting by patient cohort. Clinics evaluating a broader connected healthcare platform strategy usually make better decisions here because they assess the full patient journey, not just isolated tools.
Why does this rise to board-level priority? Because the cost of weak engagement shows up everywhere. Missed appointments leave schedule gaps. Incomplete intake slows registration and rooming. Unanswered post-visit questions drive callbacks, complaints, and avoidable revisits. Poorly designed digital tools can also create equity problems if they work well for digitally confident patients and poorly for everyone else.
Many organisations are now pairing engagement platforms with workflow automation and service operations. If you're reviewing options, it helps to look at adjacent models such as solutions for healthcare support teams, where routine coordination work is structured around responsiveness, escalation, and coverage instead of ad hoc inbox management.
The business case usually comes down to three practical outcomes:
Operational stability: Less repetitive back-and-forth, fewer manual reminders, and clearer ownership of patient communications.
Clinical continuity: Better follow-through between booking, preparation, treatment, and post-visit actions.
Financial protection: Lower leakage from no-shows, abandoned intake, delayed follow-up, and inefficient staff time.
Organisations that get results treat patient engagement technology as part of care delivery design. That matters even more as AI becomes part of the stack, because the question is no longer whether patients can use the tool. The question is whether patients helped shape it so it works safely, clearly, and at scale in a Canadian care setting.
Understanding the Building Blocks of Engagement Tech
Most buyers encounter patient engagement technology as a bundle of modules. That can make the category look messy. In practice, the strongest platforms behave like a connected toolkit with one job: help patients move through care with less confusion and less delay.
The core components that matter
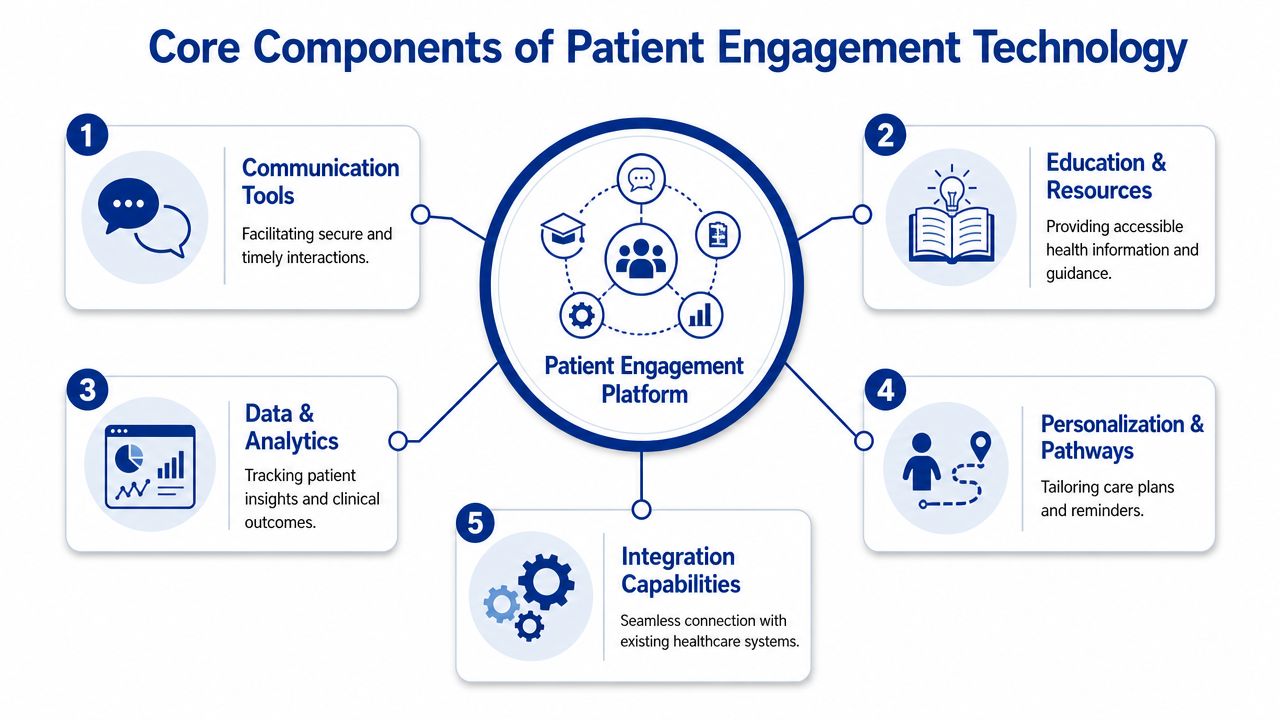
A usable engagement stack usually includes these five layers:
Communication tools: Secure messaging, appointment reminders, broadcast updates, and escalation pathways. These are the front line for reducing missed steps and confusion.
Education and resources: Condition-specific instructions, onboarding content, FAQs, and follow-up guidance. This layer helps patients act, not just receive information.
Data and analytics: Dashboards that show completion rates, message volume, adherence signals, and engagement patterns by cohort.
Personalisation and pathways: Care plans, reminders, prompts, and task sequences specific to visit type, condition, language needs, or patient preferences.
Integration capabilities: APIs, standards support, and workflow connectors that tie the engagement layer back to the EHR and operational systems.
When these pieces work together, the patient doesn't experience them as separate tools. They experience one coherent service journey.
What each tool is actually for
A patient portal is often the digital front door. It handles forms, results, scheduling, and record access. But a portal alone rarely creates strong engagement. It's too passive unless connected to reminders, customized education, and responsive communication.
Telehealth expands access, especially for follow-up, triage, and low-friction consults. Mobile apps can extend that support between visits, which matters in chronic care and ongoing care navigation. Remote patient monitoring adds another layer by bringing patient-generated data into the care process, provided the team has a workflow for acting on it.
A feature isn't useful because it exists. It's useful because someone owns the response when the patient uses it.
Analytics often gets underused. Buyers focus on whether a platform can send messages, but the stronger long-term value comes from learning which pathways patients complete, where they drop off, and which populations need another format or outreach channel.
Why integration is the non-negotiable layer
The technical foundation matters more than many non-technical buyers realise. In Canada, patient engagement architecture has increasingly centred on RESTful APIs, HL7 FHIR standards, and event-based messaging because those elements support secure interoperability and cleaner identity matching within real care workflows. For teams evaluating architecture priorities, this is closely related to broader thinking around connected healthcare platforms.
If the system doesn't integrate cleanly, staff end up double-documenting, checking multiple queues, or manually reconciling patient status. That's when “engagement” becomes administrative drag.
A practical buying lens is to ask whether the platform supports these four use cases cleanly:
| Component | What good looks like | What usually fails |
|---|---|---|
| Communication | Messages tied to care events and escalations | Generic blasts with no workflow ownership |
| Education | Relevant content delivered at the right moment | Static libraries patients never revisit |
| Monitoring | Clear thresholds and action routes | Data collection with no response model |
| Integration | Information flows into existing systems | Staff copy and paste across tools |
That's the difference between a digital channel and a functioning engagement system.
Unlocking Value Beyond the Patient Experience
The strongest patient engagement programmes don't just make patients happier. They change how the clinic runs. Better engagement reduces avoidable friction, and that creates a flywheel. Staff spend less time chasing basics, patients complete more of the right actions, and the organisation gets more capacity without adding the same level of overhead.

Clinical value shows up in timeliness and follow-through
When patients get reminders, instructions, and a direct way to ask questions, care becomes less episodic. The team can intervene earlier, clarify next steps faster, and spot disengagement before it turns into a missed appointment or an unmanaged issue.
This is especially visible in pathways where confusion is expensive. Pre-op preparation, discharge follow-up, medication reminders, prenatal support, and chronic care management all benefit when information arrives in sequence instead of in a stack of handouts.
A good example of what patients often need is structured, plain-language support around life-stage care. Resources such as discovering essential parent support illustrate how guidance, timing, and accessibility matter just as much as the content itself.
Business value is easier to defend than many teams think
The market signal is already strong. A 2021 survey found that 83% of ambulatory healthcare respondents said patient engagement solutions were critical to their organisation's financial success (North American market analysis). That's not surprising from an operational perspective. Engagement tools influence scheduling efficiency, staff workload, retention, and care continuity all at once.
Here's how the value usually appears inside a clinic or health system:
Fewer preventable gaps: Automated reminders and follow-up reduce leakage across scheduling and care plans.
Better staff utilisation: Front-desk and nursing teams spend less time on repetitive outbound contact.
Higher service consistency: Patients get standardised communication instead of depending on who happens to be on shift.
Stronger loyalty: Patients are more likely to stay with providers who make care easier to manage.
What works in practice: Tie engagement tools to one expensive operational problem first. No-shows, referral leakage, post-discharge calls, or overdue follow-up are all better starting points than a broad “digital transformation” brief.
The flywheel effect is the real payoff
A single reminder system won't transform a clinic. But a connected engagement model can. Better communication improves attendance. Better attendance improves schedule integrity. Better schedule integrity frees staff time. Staff then spend more time on higher-value patient needs, which improves experience and strengthens retention.
That's why the business case shouldn't be framed as “soft” patient satisfaction. It's a workflow, revenue, and care delivery strategy.
How to Measure Patient Engagement ROI
Most organisations make one of two mistakes when they try to measure return. They either reduce everything to software cost, or they track so many indicators that nobody can tell whether the programme is working. A practical ROI model is narrower. It connects engagement activity to operational, financial, clinical, and behavioural outcomes.
The market itself shows why disciplined measurement matters. The global patient engagement technology market is forecast to grow by USD 47.06 billion by 2029, with North America holding a 43.59% revenue share (patient engagement market forecast). Buyers are investing at scale because they expect measurable returns, not because the category sounds modern.
Start with one business problem and one baseline
Before launch, define what needs to improve. That might be appointment adherence, admin burden, follow-up completion, digital intake adoption, or time spent answering routine questions. Then capture a baseline from current operations.
If the organisation can't answer “what's broken today?”, the post-launch review will turn into opinion. A good analytics partner or internal BI team can help structure that baseline work. Teams that need a measurement framework often benefit from approaches used in healthcare data analytics solutions, where operational and clinical signals are mapped to decision points instead of dumped into a dashboard.
Use a balanced scorecard
This is the simplest way to avoid a one-dimensional ROI story.
| Domain | KPI Example | What It Measures |
|---|---|---|
| Operational | Portal activation, digital intake completion, admin call categories | Whether workflows are shifting from manual to digital |
| Financial | No-show trend, recovered appointment capacity, billing-related follow-up burden | Whether the platform is protecting revenue and reducing waste |
| Clinical | Follow-up adherence, care plan completion, escalation response timing | Whether patients are moving through care as intended |
| Engagement | Message response patterns, content completion, active patient cohorts | Whether patients are participating over time |
Not every KPI belongs in the executive report. Some matter to managers, some to clinical leads, and some to finance. Keep the top-line view short enough that leadership can act on it.
Measure value creation, not just savings
Patient engagement technology often creates value indirectly. It might not lower a line item immediately, but it can protect schedule utilisation, improve continuity, and reduce staff rework. Those are real gains.
For financial modelling, some teams use tools that help calculate your return on investment before procurement so they can compare scenarios such as automation-first reminders versus broader patient communication redesign.
Measurement advice: Review ROI at three levels. Feature adoption tells you whether the tool is being used. Workflow metrics show whether operations changed. Outcome metrics show whether that change mattered.
A final caution. Don't let the dashboard reward volume over usefulness. More messages sent is not success if patients ignore them. Better engagement is visible when the right patients complete the right actions with less staff intervention.
A Practical Roadmap for Implementation
Implementation fails when leaders treat it as a software rollout instead of a care redesign project. The tool matters, but the core work sits in workflow decisions, integration planning, privacy controls, and patient onboarding.
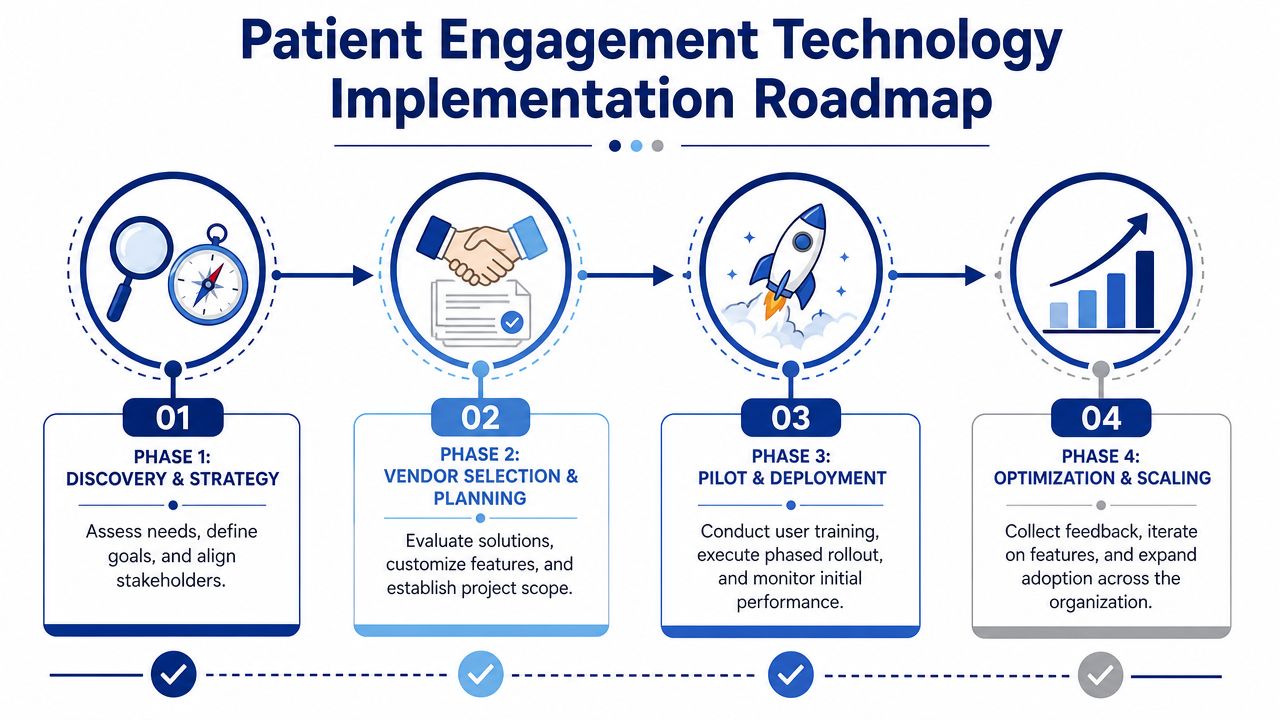
Phase one and two need operational clarity
Start by choosing a use case with clear pain. Missed appointments, referral coordination, post-visit communication, or chronic care follow-up are common entry points because the workflow is visible and the cost of failure is easy to explain.
Then map the current state in plain terms:
Who initiates contact: Front desk, nurse, care coordinator, or automated trigger.
What systems are touched: EHR, scheduling platform, call centre queue, messaging tool.
Where delays happen: Approval bottlenecks, incomplete forms, unanswered reminders, manual transcription.
Which patients struggle most: Older adults, low-literacy users, rural patients, or patients with complex care journeys.
This stage often exposes that the problem isn't “lack of a platform.” It's unclear ownership.
Interoperability and compliance come before scale
In Canada, the technical architecture matters because interoperability determines whether the platform supports real care delivery or creates another disconnected layer. A framework based on HL7 FHIR has been identified as critical, and this architecture is associated with a 20 to 30% reduction in no-show rates when communication is synchronised between front-desk operations and care teams (Canadian framework for patient engagement in health technology assessment).
That finding is useful because it links architecture to operational outcome. Integration is not an IT preference. It is part of the business case.
Security planning also needs to be explicit. Buyers should require a clear account of data flows, access controls, consent handling, auditability, and how the vendor supports Canadian privacy obligations. Cross-border hosting, subcontractors, and AI processing need review before procurement is complete, not after launch.
Don't approve a patient engagement rollout until clinical leads can describe what happens when a patient replies, escalates, misses a step, or stops engaging entirely.
Pilot narrowly and redesign around real use
A good pilot is small enough to monitor but important enough to matter. One clinic, one specialty, or one care pathway usually works better than an enterprise-wide launch.
Use the pilot to test:
Staff workflow fit: Can teams act on alerts and messages without creating hidden work?
Patient comprehension: Do patients understand what the tool is for and when to use it?
Equity issues: Are there patients who can't use the channel reliably?
Escalation paths: Does urgent communication route correctly?
Then refine scripts, reminders, education formats, and ownership rules before scaling. Most implementation risk appears in those details, not in the demo environment.
Choosing the Right Solution for Your Needs
The right platform depends less on organisation size than on service model. A small primary care clinic may need reminders, intake, and secure messaging. A hospital programme managing cardiology follow-up may need remote monitoring and escalation workflows. A digital health startup may need a branded experience with flexible APIs and patient-specific content pathways.
That's why feature comparison sheets can mislead buyers. Two vendors may both offer messaging and portals, but only one may fit your workflow, privacy posture, and patient population.
Three common buying scenarios
A community clinic usually needs simplicity. Staff won't have time to manage a complicated admin console, and patients won't tolerate a difficult login flow. In that setting, reliable reminders, straightforward digital forms, and message routing matter more than a long innovation roadmap.
A regional provider group often needs coordination across teams. The issue isn't whether the tool can send notifications. It's whether the scheduling team, clinicians, and care coordinators can work from the same status signals.
A specialised programme serving remote populations has a different priority. The main risk is exclusion. Research on rural and remote Canada highlights the digital divide as a primary barrier, which means buyers should pay close attention to inclusivity, connectivity constraints, and offline-friendly design (digital divide in rural and remote Canada).
A practical vendor checklist
Use this checklist during selection:
Interoperability: Ask how the platform connects to your EHR, scheduling system, and identity workflows.
Workflow ownership: Verify who handles inbound messages, escalations, and unresolved patient tasks.
Inclusivity features: Look for multilingual support, low-friction interfaces, and options that work when connectivity is inconsistent.
Compliance fit: Review privacy controls, hosting approach, audit trails, and AI governance if automation is involved.
Support model: Ask how implementation, training, and post-launch optimisation are handled.
The best buying decision usually comes from matching one solution to one operational problem first. If the vendor can't describe how the product will work in your actual care pathway, keep looking.
The Next Frontier: Custom Development and AI
Off-the-shelf platforms are useful when your needs match common workflows. They're less useful when your organisation has specialised pathways, multiple stakeholder groups, or patient populations with very different literacy, language, and access needs. That's where custom development becomes strategic rather than cosmetic.
Custom work lets a team control the patient journey more tightly. You can shape intake, messaging logic, educational sequences, staff routing, and reporting around your actual operating model instead of adapting your operations to a vendor's default assumptions. For organisations exploring that path, broader thinking around AI integration in software development and operations is especially relevant because AI changes not just the interface, but the underlying workflow and governance requirements.
AI is useful only if patients shape it
The biggest mistake in AI-driven patient engagement is treating patient input as a final-stage usability check. Research in this area argues for a stratified, layered approach across the AI lifecycle and warns that one patient does not represent all patients (research on stratified patient engagement in AI). That matters because biased training assumptions, narrow testing groups, and weak literacy support can produce tools that technically function but miss the people they're meant to help.
A better model looks like this:
Core patient partners: A small, consistent group involved across design, review, and iteration.
Targeted patient cohorts: Different groups consulted at specific stages based on condition, language, age, geography, or digital literacy.
Operational staff input: Front-desk teams, nurses, and care coordinators who know where patients get stuck.
Where custom development earns its keep
This is especially relevant for AI-supported triage, care navigation, reminders, symptom check-ins, and patient support chat flows. These systems need guardrails, escalation logic, and language that fits real patient behaviour.
One example in this space is Cleffex Digital Ltd, which develops secure custom software and healthcare AI tools such as chatbots for scheduling, reminders, symptom triage, and patient support. That kind of build approach makes sense when an organisation needs tighter control over workflow, branding, integration, and compliance than an off-the-shelf product can offer.
The future of patient engagement technology isn't more features. It's better-designed participation. The organisations that win won't just deploy AI. They'll involve the right patients, at the right moments, in shaping how AI serves care.
If your clinic, health system, or healthcare startup needs patient engagement technology that fits real workflows, privacy requirements, and AI use cases, Cleffex Digital Ltd can help assess the gap between off-the-shelf tools and custom development. The practical starting point is simple: define the patient journey you need to improve, map the workflow around it, and build from there.







