



Administrative work consumes a large share of healthcare operations. For Canadian clinics and hospitals, that pressure shows up in referral bottlenecks, duplicate data entry, billing delays, and staff time lost to systems that were never designed to work well together. Automation matters because those inefficiencies hit access, margin, and clinician capacity at the same time.
Healthcare automation software should be treated as an operating model decision, not a software purchase. Leadership teams need to ask a harder question than whether automation can save time. They need to decide which workflows should be standardised first, which systems must exchange data cleanly, and how the rollout will satisfy provincial privacy and documentation requirements without disrupting care delivery.
This is the point where many projects stall.
The problem is rarely ambition. The problem is integration discipline. A scheduling bot, intake workflow, or claims automation tool can look impressive in a demo and still fail in production if it cannot work with a legacy EMR, support local consent practices, or fit the way front-desk staff and clinicians move through the day. Teams that ignore those realities end up adding another layer of operational friction.
Many articles reduce the topic to AI promises and generic efficiency claims. That is not enough for a hospital or clinic leadership team to build a business case. A more insightful discussion begins with workflow design, data handoffs, auditability, procurement constraints, and the practical work of modernising healthcare operations across fragmented systems.
This article focuses on that practical layer. It examines how healthcare automation software fits into Canadian delivery environments, where interoperability with legacy platforms, provincial compliance, and implementation sequencing decide whether automation produces measurable relief or expensive rework.
The Revolution in Clinic and Hospital Operations
Analysts estimate that North America accounts for a large share of healthcare automation spending, and earlier market data also pointed to major annual savings tied to reducing administrative waste. Leadership teams should read that trend correctly. Administrative work is no longer a background issue. It is a direct constraint on access, margin, staff retention, and clinical capacity.
Healthcare automation software has moved from “innovation” to “infrastructure” for a simple reason. Manual clinic and hospital operations break down under scale. They create delays in intake, slow down claims processing, increase documentation burden, and make it harder to maintain consistent audit trails across multiple systems.
In Canadian organisations, the pressure is even more specific. Hospitals and clinics rarely start from a clean technology environment. They are working with legacy EMRs, departmental tools, provincial billing rules, privacy obligations, and workflows built around years of local workarounds. Any automation plan that ignores those realities will create more friction, not less.
Use a strict test. If a process is repetitive, rules-based, high-volume, and needs a clear audit trail, treat it as an automation candidate until someone can justify keeping it manual.
That usually puts appointment intake, eligibility checks, referral routing, claims follow-up, charge capture support, prior authorisation steps, discharge communication, and document handling near the top of the list. Clinical workflows also belong in scope, but leadership should be selective. Note support, triage routing, image workflow assistance, and alert distribution can deliver value, but only if the software fits clinician practice and exchanges data cleanly with the systems already in use.
The biggest buying mistake is treating automation as one product category. It is not. It is an operating layer made up of workflows, integrations, rules engines, communication tools, and governance controls. Leadership teams that understand this make better decisions about sequencing and procurement. They avoid the common outcome of buying a polished front-end tool that cannot work properly with the EMR, billing process, or consent model behind it.
Start with an operational review, not a vendor shortlist. Map where staff re-enter data, where handoffs fail, where compliance checks rely on memory, and where legacy systems force avoidable manual work. That is the practical basis of modern healthcare operations improvement. If automation does not improve throughput, accuracy, compliance, or clinician time, it should not make the roadmap.
Understanding the Healthcare Automation Ecosystem
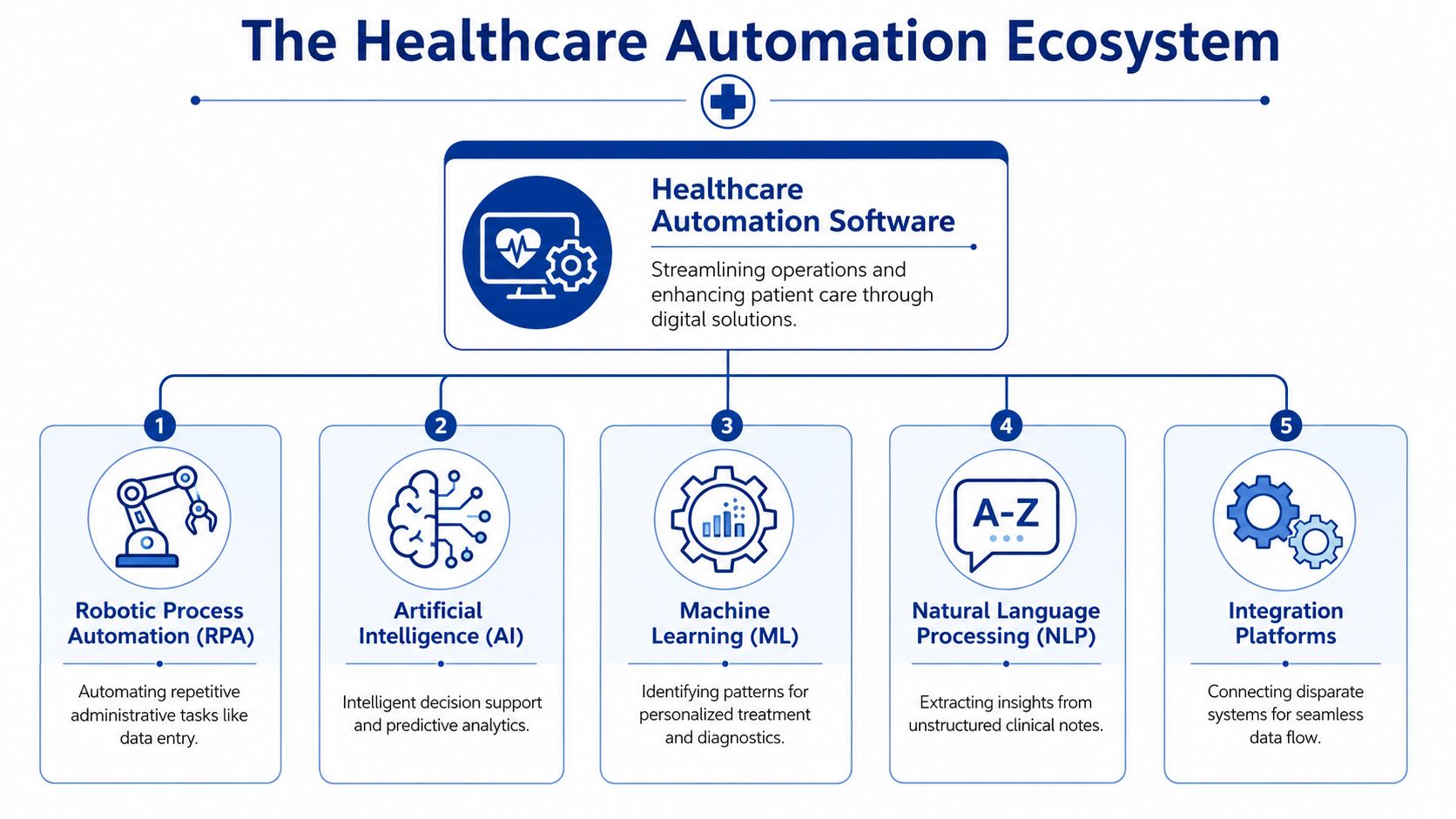
Think of healthcare automation software as the digital nervous system of a clinic or hospital. It senses what's happening, routes information where it needs to go, triggers actions based on rules, and reduces the need for staff to re-enter the same data across multiple systems.
That description matters because many buyers still think automation means one thing. It doesn't. It's a connected ecosystem of tools that handle different parts of operations.
Administrative automation
Most organisations should begin with administrative automation, as process waste is easiest to spot and fix in this area.
Common examples include:
Scheduling workflows: online booking, reminders, cancellations, waitlist logic, and follow-up routing.
Revenue cycle tasks: Eligibility verification, claims status checks, coding support, and payment posting hand-offs.
Document handling: Intake forms, referral packets, consent processing, and records requests.
Communication flows: Patient messages, appointment confirmations, and staff task routing.
This category usually delivers the first visible improvement because staff can feel the workload shift. The front desk spends less time toggling between screens. Billing teams stop copying data manually. Managers gain a clearer view of bottlenecks.
Clinical automation
Clinical automation supports care delivery directly or indirectly. It doesn't replace clinical judgement. It reduces friction around it.
Examples look different from admin tools:
| Clinical area | What automation typically does |
|---|---|
| Documentation | Structures notes, extracts key details, supports drafting |
| Diagnostics support | Flags patterns, surfaces anomalies, prioritises review queues |
| Care coordination | Routes orders, referrals, discharge instructions, and follow-up tasks |
| Monitoring workflows | Triggers alerts and escalations based on incoming patient data |
A useful buying test is this: can the software improve a workflow without forcing clinicians to become data-entry clerks for the software itself?
That's the line many vendors still fail.
The ecosystem also depends on the systems in between. Integration middleware, APIs, identity controls, audit logs, and workflow orchestration tools often matter more than a flashy user interface. If those foundations are weak, your automation layer becomes brittle fast.
If your organisation is evaluating multiple systems, look at them through the lens of connected healthcare platforms. Good automation software doesn't just perform a task. It fits into a broader architecture where patient, operational, and financial data can move cleanly across systems.
Impactful Use Cases of Automation in Healthcare
The strongest business case for healthcare automation software comes from concrete workflow change, not abstract promises. Leaders need to ask what work is currently delayed, duplicated, error-prone, or dependent on staff heroics. That's where automation pays off.
Healthcare organisations integrating advanced analytics and automation see an average ROI of 147% within three years, and AI-scribe deployments reduce physician documentation time by 40 to 45%, according to TempDev's healthcare AI statistics roundup. Those numbers matter because they connect automation to both financial return and clinical time recovery.
Before and after in revenue cycle operations
Before automation, a billing or patient access team often worked from inboxes, spreadsheets, payer portals, and phone calls. Eligibility checks get repeated. Claims statuses are chased manually. Missing data creates avoidable rework.
After automation, the same team can route repetitive checks through rules-based workflows, trigger work queues based on claim status changes, and standardise exception handling. Staff still work the hard cases. They stop wasting time on the obvious ones.
That's why the revenue cycle is usually one of the best early targets. It has volume, repeatability, and direct financial impact.
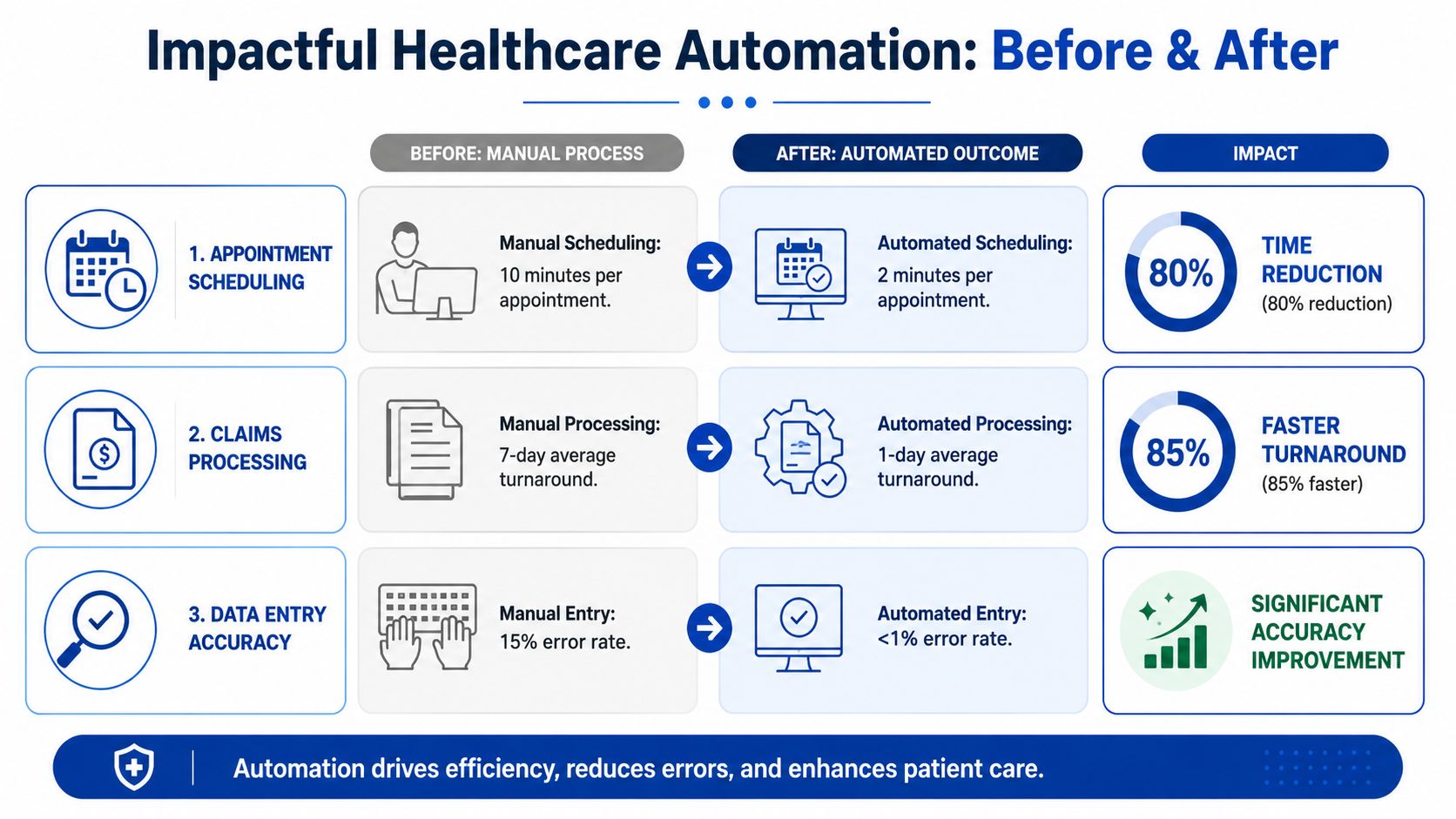
Before and after in clinical documentation
Before automation, clinicians finished patient interactions and then faced another job. Notes, forms, coding details, hand-offs, and follow-up tasks pile up after the visit. That creates delay, fatigue, and inconsistency.
After a strong documentation support workflow is introduced, the clinician reviews and confirms rather than composing everything from scratch. That's a very different operating model. It preserves oversight while reducing the clerical burden that drags down capacity.
The real gain isn't just faster note creation. It's getting clinical attention back into the encounter instead of into the keyboard.
Before and after in diagnostics and care coordination
In imaging, pathology, and triage-heavy settings, automation can prioritise queues, surface suspicious findings for review, and push the right case to the right team sooner. In discharge and referral management, it can route tasks automatically, generate required communication steps, and make sure open loops are visible.
These aren't glamorous wins, but they matter. Delays in routing and follow-up cause operational drag across the entire organisation.
A practical shortlist of high-value use cases looks like this:
Patient access automation: Registration, intake, document capture, and scheduling logic.
Claims and billing workflows: Repetitive revenue cycle tasks that follow stable business rules.
Clinical note support: Documentation drafting and structured data capture under clinician review.
Referral and discharge orchestration: Task routing across departments and external partners.
Diagnostic queue support: Prioritisation and anomaly surfacing in high-volume review settings.
If you want a grounded view of where AI fits into these workflows, AI-powered healthcare solutions offer a practical lens. The leadership issue isn't whether AI is present. It's whether the workflow around it is safe, integrated, and worth adopting.
Core Technologies Powering Modern Medical Software
Most vendor conversations overload buyers with jargon. Strip that away, and the underlying technologies are straightforward. Each one solves a different class of problem. If you don't separate them, you'll buy tools that sound advanced but don't fit your actual needs.

RPA for repetitive and rules-based work
Robotic Process Automation, or RPA, is the blunt instrument of healthcare automation software. That's not a criticism. It's useful because many hospital and clinic workflows are still repetitive and highly structured.
RPA is best when the process:
Follows fixed rules: The same trigger leads to the same next action.
Touches multiple systems: Staff currently copy and paste across applications.
Needs an audit trail: Every step should be traceable.
Has predictable exceptions: Unusual cases can be kicked to a human queue.
Think eligibility checks, claims status pulls, patient onboarding hand-offs, or moving data between older systems that don't integrate well natively.
AI and ML for judgment support
Artificial Intelligence and Machine Learning become useful when the problem is less about repetition and more about interpretation, prediction, or prioritisation.
They help when software needs to:
| Technology | Best suited for | Typical healthcare use |
|---|---|---|
| AI | Decision support and pattern detection | Triage support, imaging assistance, workflow recommendations |
| ML | Learning from historical data | Risk scoring, forecasting demand, identifying recurring operational patterns |
Many buyers often get distracted. AI isn't automatically the better answer. If your billing team is still manually checking standard claim statuses, you probably need process automation before predictive models.
The practical lesson from Happy Billing RCM expertise is that revenue cycle improvement often starts with disciplined workflow automation, not with buying the most advanced AI pitch in the room.
NLP and integration platforms for real-world usability
Natural Language Processing, or NLP, matters because healthcare runs on unstructured language. Notes, messages, referrals, discharge summaries, and patient communications don't arrive in neat database rows.
NLP helps systems extract meaning from that text so organisations can classify information, draft structured outputs, route work correctly, and reduce manual review effort.
Then there's the category buyers routinely underestimate: integration platforms. These tools connect EMRs, billing systems, labs, repositories, and third-party services. Without that plumbing, every automation layer becomes another silo.
Buy technology in this order. Workflow fit first, integration second, model sophistication third.
That ordering will save you money and political pain.
One practical example in the Canadian market is Cleffex Digital Ltd, which builds custom software and AI-enabled healthcare workflows that can be aligned with existing enterprise systems rather than forcing a one-size-fits-all platform approach. That model is often more realistic for organisations with mixed legacy environments.
Integrating Software with Canadian Healthcare Systems
Good automation projects separate from expensive disappointments through their interoperability. In Canada, healthcare automation software lives or dies on interoperability. If it can't exchange data with your EMR, payer workflows, provincial repositories, and internal operational systems, it won't reduce burden. It will just move the burden around.
The core requirement is clear. In Canada, healthcare automation software should be built around HL7 and FHIR so data can move across EMRs, payer platforms, and provincial repositories without manual re-entry while preserving privacy.
Why standards-first beats feature-first
Many healthcare buyers still choose software based on the demo. That's backwards. The demo shows a controlled environment. Your organisation runs on exceptions, mixed vendors, local customisation, and historical workarounds.
A standards-first approach matters for several reasons:
Legacy EMRs aren't going away soon: New automation has to coexist with them.
Provincial workflows vary: What works in one operating environment may need adaptation in another.
Data quality depends on clean exchange: Duplicate entries create inconsistency and risk.
Privacy controls must travel with the workflow: Access, auditability, and traceability can't be bolted on later.
That's why I advise leadership teams to reject any vendor that treats integration as a post-contract detail. It should be central in procurement, architecture review, and rollout planning.
What Canadian teams should demand up front
Don't ask a vendor whether they “support interoperability”. Ask how.
Use a checklist like this:
API capability: Can the platform work through modern APIs rather than only flat-file workarounds?
HL7 and FHIR readiness: Which standards are implemented, and for which workflow types?
Role-based access control: Can you limit access by job function and workflow context?
Audit logging: Can you see who accessed, changed, or transmitted data?
Exception handling: What happens when source data is incomplete, duplicated, or mismatched?
Workflow adaptability: Can the system be configured for local and provincial differences without custom rebuilds?
If a vendor needs your staff to manually repair data movement every day, you have not automated anything meaningful.
Compliance is operational, not legal theatre
Canadian privacy obligations are often discussed as a legal review item. That's too narrow. Compliance has to show up in the day-to-day operation of the software. Staff should know what is logged, what is restricted, what is retained, and how workflows handle sensitive data.
PIPEDA and provincial obligations matter, but leadership teams shouldn't reduce compliance to policy language in a sales deck. They should test whether the software enforces privacy in routine use. That means permission controls, logging, secure transmission paths, and clear handling of third-party integrations.
The broader procurement reality is also worth stating plainly. Buyers in Canada usually care less about broad feature lists than about implementation friction. They want to know how hard the software is to fit into real operating conditions. That is the correct priority.
A Strategic Roadmap for Software Implementation
The safest way to implement healthcare automation software is to treat it as an operational transformation programme, not a software launch. Most failures happen because organisations buy too much, too quickly, with weak workflow definition and vague ownership.
A disciplined rollout is slower at the start and faster in the long run.
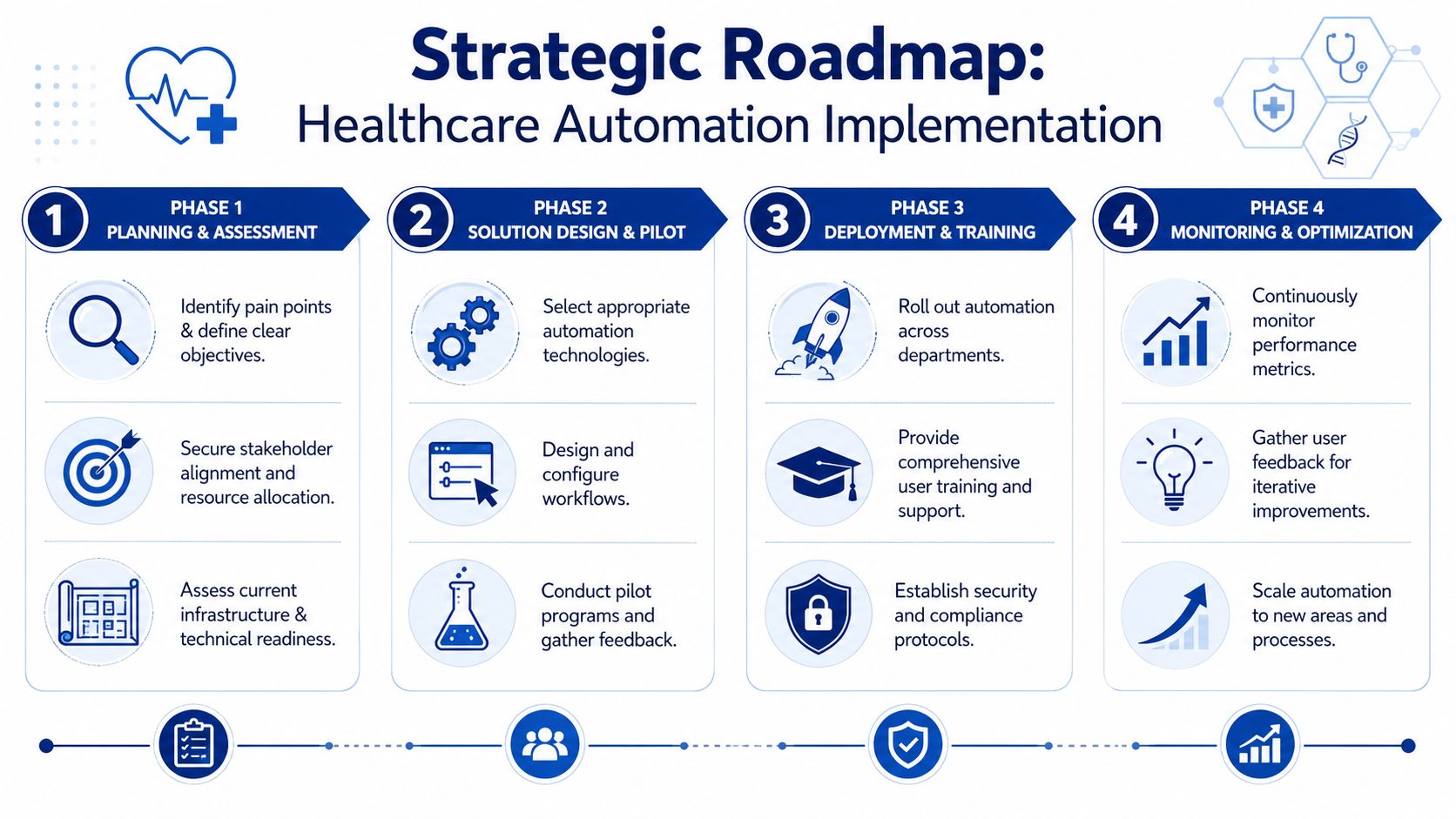
Phase one planning and assessment
Start with process selection, not vendor selection. Identify where staff are losing time, where errors recur, and where delays hit patient service or cash flow.
Your first target should usually have these traits:
High volume: Enough repetition to justify design effort.
Clear rules: Stable decision logic that can be standardised.
Cross-functional pain: Visible burden across admin, clinical, or finance teams.
Measurable outcomes: Cycle time, backlog reduction, staff time recovered, or improved completion rates.
Don't pick the most politically visible process. Pick the one that is painful, common, and fixable.
Phase two: Solution design and vendor evaluation
Once you know the workflow, then evaluate the tools. At this stage, buyers often overvalue features and undervalue implementation fit.
Use vendor criteria that reflect reality:
| Evaluation area | What to check |
|---|---|
| Integration | EMR connectivity, API maturity, HL7/FHIR support, audit trails |
| Workflow design | Configurable rules, exception handling, approvals, local adaptation |
| Security and privacy | Access controls, logging, data handling controls, hosting model |
| Adoption support | Training approach, change management, admin usability |
| Scalability | Can the same platform expand to adjacent workflows later |
A good vendor should be able to map your current process, identify where automation belongs, and explain where human review must remain. If they can't do that, they're selling software, not a solution.
Phase three pilot and phased rollout
Run a contained pilot. Don't start enterprise-wide unless your environment is unusually simple, and most aren't.
A sensible pilot has:
A single workflow boundary
Named operational owners
Defined exception paths
User feedback loops
A rollback plan
Pilot the process with the highest learning value, not the one with the lowest risk. You need proof that the model works under normal operational pressure.
Roll out in phases after the pilot proves workflow fit, integration stability, and staff acceptance. Sequence departments based on readiness, not hierarchy.
Phase four measurement and iteration
Post-launch, measure whether the system changed the work. Usage metrics alone don't tell you enough. You need operational metrics tied to the original problem.
Track items such as:
Process speed: Whether routine work is moving faster.
Manual touchpoints: Whether staff are still doing duplicate entry or rework.
Exception volume: Whether source systems or rules need adjustment.
User confidence: Whether staff trust the output enough to rely on it.
Expansion readiness: Whether adjacent workflows can now be automated with lower effort.
This is also where leadership should decide whether to keep extending a vendor platform, build custom components, or add orchestration tools around core systems. That decision depends on architecture, not vendor marketing.
Preparing for the Next Wave of Healthcare Innovation
The best reason to invest in healthcare automation software isn't speed alone. It's focus. Organisations need clinicians focused on care, finance teams focused on exceptions that matter, and operations teams focused on improving access rather than repairing broken hand-offs.
That's why automation should be framed as workforce augmentation, not staff replacement. Good systems remove repetitive admin, standardise predictable actions, and make expert time more valuable. Bad systems just move clerical work onto different people.
The next wave will push further into orchestration. More workflows will combine structured automation, language processing, predictive support, and integrated data models. That makes your current architectural choices more important than ever. If your data foundation is fragmented, future AI tools won't deliver much. If it's standardised and accessible, you'll have options.
For leadership teams thinking ahead, work on interoperability and data structure now. Resources on leveraging OMOP for AI development are useful because they show how standardised clinical data models can support more advanced analytics and AI without rebuilding everything from scratch later.
Choose a technology partner that understands healthcare operations, not just software delivery. In this market, implementation discipline is the strategy.
If your organisation is evaluating healthcare automation software and needs a practical build-versus-buy assessment, integration planning, or a phased implementation roadmap, Cleffex Digital Ltd can help scope secure, compliant solutions for Canadian healthcare environments.







