



Canada's digital health market was valued at about CAD 5.3 billion in 2024 and is projected to reach roughly CAD 10.6 billion by 2030. Growth at that pace creates pressure in a system that does not operate as one market. In Canada, a platform decision is rarely just a tooling decision. It affects how an organisation handles provincial privacy rules, hospital procurement realities, data residency expectations, and integration work across separate health authorities and vendor ecosystems.
I see the same pattern repeatedly. Teams start with familiar DevOps fixes: add CI/CD, standardise Kubernetes, automate infrastructure. Those steps help, but they do not solve the harder Canadian problem. A product may need to satisfy PIPEDA, align with provincial health privacy requirements, support different hosting constraints by customers, and prove auditability to risk teams that do not share the same interpretation of acceptable controls.
That is why healthcare platform engineering matters here. It gives delivery teams a repeatable operating model for building and running software under uneven regulatory and commercial conditions. Without that model, every new application becomes a custom negotiation between engineering, security, privacy, legal, and procurement.
The cost shows up in missed release dates, duplicated controls, inconsistent logging, and cloud spend hidden inside one-off exceptions.
Many healthcare organisations still work this way. One team provisions cloud resources by hand. Another copies a deployment pipeline from an earlier project. Privacy reviews live in spreadsheets. Audit evidence gets assembled late, under deadline, by people who did not design the system in the first place. That approach may be tolerable for an internal pilot. It does not hold up when an organisation has to scale across provinces, support multiple care settings, or pass customer security review without rebuilding the same control set each time.
In practice, the trade-off is not speed versus compliance. Instead, the trade-off is whether compliance is built into the platform early, with some upfront investment and tighter standards, or paid for later through rework, slower sales cycles, and operational inconsistency. In Canada's fragmented health market, platform engineering is how teams reduce that drag and create a path to scale.
The New Foundation for Digital Health
In Canadian healthcare, delivery often breaks down at the provincial boundary, the privacy review queue, or the point where a product team needs production access. That is why platform engineering has become a foundation issue, not an infrastructure preference. It gives organisations a repeatable way to ship digital health products across a market shaped by PIPEDA, provincial privacy laws, public sector procurement, and uneven technical maturity across providers.
The practical problem is straightforward. If every delivery team has to assemble its own cloud architecture, identity model, deployment pipeline, logging standard, and audit approach, the organisation pays for the same decisions many times. It also accepts avoidable variation in controls that should be standard.
That cost shows up in places where executives and engineering leaders both feel. Releases slow down. Privacy and security reviews get longer. Support teams inherit systems with inconsistent telemetry. Cloud spend rises because custom environments and one-off integrations are harder to govern.
Why the Old Project Model Struggles
The old project model usually fails in three places:
Delivery speed: Teams build their own stack and approval path for each product.
Compliance timing: Controls are reviewed late, when design changes are expensive.
Operational consistency: Backup policies, alerting, access patterns, and audit trails differ across systems.
In healthcare, those gaps create business risk, not just technical debt. A delayed release can stall a hospital deployment. An inconsistent access model can complicate a privacy assessment. Weak audit design can lengthen enterprise sales cycles because customer security questionnaires expose differences between teams.
Practical rule: If every application team has to solve security, deployment, and auditability from scratch, you have no engineering advantage. You have repeated operational risk.
Why a Platform Changes the Economics
A platform changes the cost profile by turning repeated engineering work into a shared product. Teams use approved environments, reference deployment patterns, identity services, integration building blocks, and policy guardrails through self-service workflows. That removes a large share of the work that does not differentiate the product but still has to be done properly.
In Canada, this matters because the market is fragmented by province, care setting, buyer expectations, and regulatory interpretation. A virtual care product, a hospital workflow tool, and a patient data service may all face different review processes even when they rely on similar technical controls. Standardisation helps contain that variance. It gives teams a common operating base so they can spend time on clinical workflows and customer requirements instead of rebuilding logging, access controls, and release processes.
The result is tighter control with less manual effort. That is the foundation digital health teams need if they want to move at a reasonable pace without losing control of compliance, reliability, or cost.
Defining Healthcare Platform Engineering
Healthcare platform engineering is the practice of building an internal product that gives software teams a secure, compliant, reusable way to develop, deploy, and operate healthcare applications. The key phrase is internal product. A platform isn't just shared infrastructure. It has users, service boundaries, documentation, support expectations, and a roadmap.
A useful analogy is city infrastructure. Developers build the houses, clinics, and office towers. The platform team builds the roads, power lines, water system, zoning rules, and inspection processes that let those buildings exist safely at scale. If the city gets the core infrastructure right, builders move faster without making the whole environment unstable.
What Makes It Different From Generic Platform Engineering
Generic platform engineering often centres on developer productivity alone. Healthcare platform engineering has to do more. It must be assumed that sensitive data, regulated workflows, and audit obligations are present from the first design decision.
That changes the design priorities:
Compliance is built in: Access patterns, encryption defaults, logging, and approval workflows can't be optional extras.
Data interoperability matters: Platforms need standard ways to connect EHRs, labs, devices, claims, and administrative systems.
Operational evidence matters: Teams must be able to show what changed, who accessed what, and how a system behaved over time.
The Paved Path Concept
The most effective platforms don't try to support every possible workflow on day one. They create a paved path. That usually includes a deployment template, identity model, secrets handling, API gateway conventions, observability defaults, and pre-approved infrastructure modules. Product teams can still request exceptions, but the normal route is fast because it has already been secured and documented.
A healthcare platform succeeds when developers choose it because it removes friction, not because governance forces them onto it.
In practice, that means the platform should expose services that developers need: environment creation, CI/CD templates, event pipelines, governed data access, standard API patterns, and run-time policy enforcement. It should also hide work they shouldn't be repeating, such as certificate handling, baseline monitoring, and control mapping for internal reviews.
Where Canadian Requirements Change the Design
Canadian healthcare organisations don't operate in a single regulatory container. PIPEDA matters, but provincial laws, data residency expectations, procurement constraints, and public-sector assurance requirements often matter just as much. That's why a healthcare platform can't just be a repackaged DevOps toolkit. It needs policy-aware defaults, clear tenant boundaries, and data handling patterns that fit a multi-jurisdiction environment.
Key Business Value and Compliance Drivers
The strongest business case for healthcare platform engineering isn't “developers like it more,” although they usually do. The stronger case is that it turns compliance and delivery into a repeatable system instead of a sequence of one-off negotiations.
Across Canadian health systems, electronic health records and connected clinical systems are now widespread, and Canada Health Infoway reported that nearly all hospitals and the vast majority of primary care settings have adopted EHR-related capabilities, according to this published review of digital health adoption in Canada. Once that level of digital adoption exists, the operational burden shifts. The challenge is no longer whether systems are digital. The challenge is whether teams can govern, integrate, and evolve them safely.
The Executive-Level Value
Leaders usually care about three outcomes:
| Concern | What the platform changes |
|---|---|
| Speed | Teams launch new services on standard foundations instead of starting from zero |
| Risk | Security and audit controls move into reusable pipelines and runtime policies |
| Cost | Shared services reduce duplicated tooling, duplicated integrations, and duplicated operational work |
The true value of platform investment becomes apparent. A team that ships on a common path spends less effort negotiating infrastructure patterns and more effort building the workflow that matters to clinicians, staff, or patients.
Compliance Stops Being a Late-Stage Bottleneck
In many organisations, compliance still behaves like a final gate. A project reaches implementation, then someone asks whether logging is sufficient, whether access reviews are traceable, whether encryption is enforced consistently, or whether third-party dependencies meet internal standards. By then, the architecture is already difficult to change.
A better model pushes those controls into the platform. Teams inherit guardrails through templates, policy as code, standard secrets management, and mandatory observability. For security leaders, a practical companion to this thinking is understanding the NIST Cybersecurity Framework, because it helps teams organise controls in a way that is easier to operationalise across shared services.
Speed Without a Compliance Argument Is Fragile
Healthcare teams sometimes frame compliance and delivery speed as opposites. In practice, weak compliance engineering slows delivery. Teams pause for manual reviews, rework integrations, and debate exceptions. Strong platform design reduces those loops by settling foundational decisions early.
That's also why many organisations benefit from a more deliberate compliance-driven software development approach. It aligns architecture, engineering, and audit expectations before product teams are buried in implementation details.
Compliance is cheaper when it is a property of the platform than when it is a checklist attached to each release.
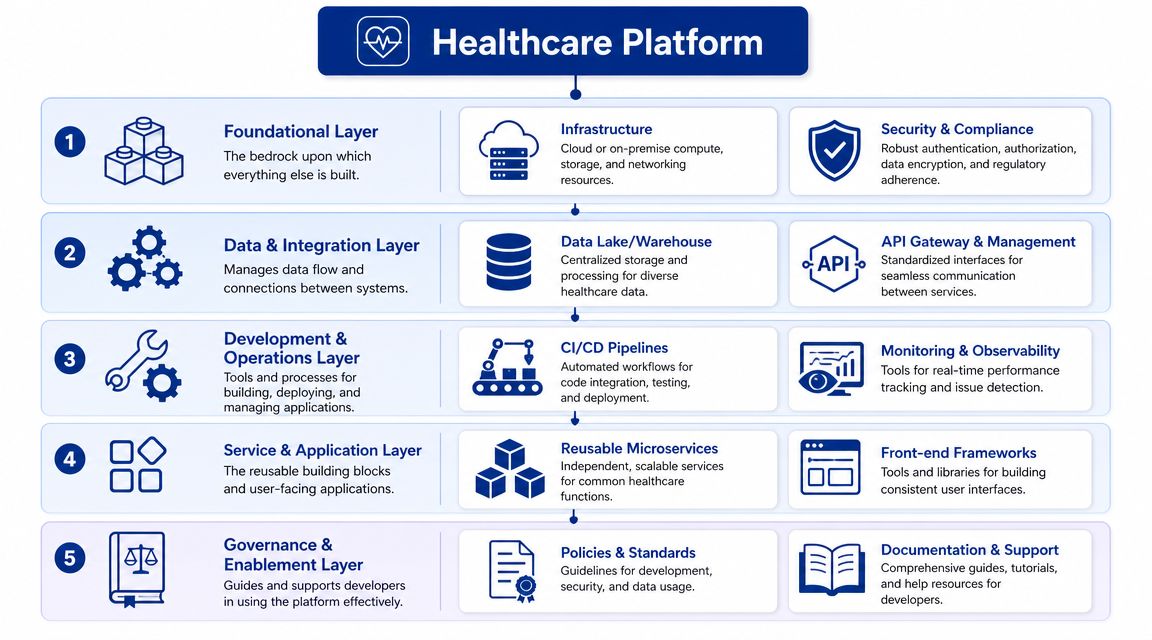
Core Components of a Healthcare Platform
A healthcare platform becomes useful when it gives delivery teams a reliable path from idea to production. The core components below are the pieces that usually make that possible. They're tightly connected. If one is weak, the others carry more weight than they should.
Canadian care delivery and analytics environments routinely pull from EHRs, medical devices, insurance databases, and laboratory systems, so the platform layer has to reconcile heterogeneous schemas, identity matching, and access control before downstream apps can reliably use the data. That's why the first component is data, not deployment.
Unified Data Platform
Without a governed data layer, every application team creates its own mapping logic, access workflow, and exception handling. That leads to inconsistent patient identity resolution, duplicated transformations, and hard-to-audit movement of sensitive records.
A usable platform should provide:
Governed ingestion paths: Standard connectors and ingestion patterns for common source systems.
Canonical models where possible: Not a fantasy of total standardisation, but a shared baseline for recurring entities and events.
Controlled data access: Teams request scoped access instead of reaching directly into operational systems.
API and Integration Layer
The API layer sits between internal services, external systems, and developer teams. It's where versioning, authentication, throttling, and contract discipline become operational rather than aspirational.
Some organisations skip this and let teams integrate directly. That works until the second or third consumer arrives. A central API pattern keeps the platform stable when applications change at different speeds.
Identity and Access Management
Identity is where many healthcare platforms fail. They authenticate users, but they don't model roles, organisational boundaries, service identities, or delegated access well enough for clinical and administrative workflows.
What works better is a layered approach:
Workforce and customer identity are separated cleanly.
Service-to-service trust is managed centrally.
Fine-grained authorisation is applied close to the data and API boundaries.
Security Toolchain and Auditability
Security tooling should be part of the developer path, not a parallel process. That includes dependency scanning, secret detection, image controls, encryption standards, policy checks, and audit log collection. If teams must assemble those pieces manually, adoption will fragment.
A connected architecture often benefits from reference patterns for integration-heavy systems, such as these perspectives on connected healthcare platforms, because the hard part isn't just connecting systems. It's doing so with governance that survives scale.
Observability and Delivery Automation
Observability in healthcare needs more than CPU and memory dashboards. Teams need traceability across workflows, integrations, queues, user actions, and policy decisions. Logs must be useful for operations and for retrospective review.
CI/CD and Infrastructure as Code complete the path. A good platform gives teams approved templates for building, testing, provisioning, and releasing. The trade-off is clear. Standardisation limits architectural improvisation, but it pays back in reliability and supportability.
Reference Architectures and Technology Stacks
A reference architecture matters because it prevents endless re-litigation of the same platform choices. It doesn't mean every team must use the same tool for every job. It means the organisation agrees on how workloads, data, identity, and controls fit together.
The most practical pattern for healthcare platform engineering is a layered architecture with a control plane, a shared data and integration layer, and product-facing workloads running on standard runtime services. In cloud-native environments, that often means container orchestration for application workloads, managed identity services, centralised secrets handling, policy enforcement in CI/CD, and a separate analytics or data platform for governed processing.
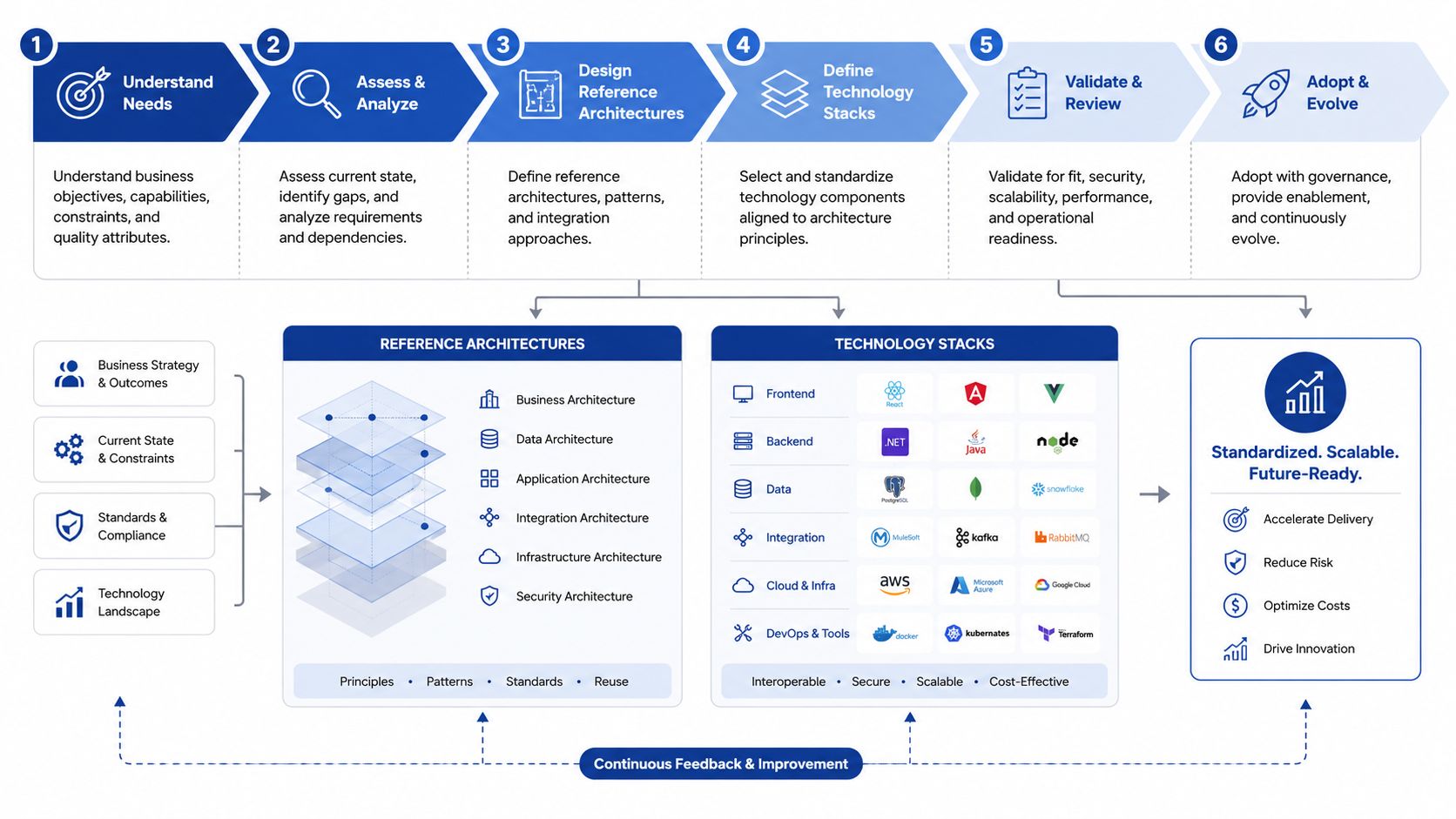
A Practical Stack Pattern
One representative stack might look like this:
| Layer | Common choices |
|---|---|
| Runtime | Kubernetes or managed container platforms |
| Infrastructure | Terraform for provisioning, cloud-native networking and storage |
| Identity | Enterprise identity provider plus workload identity for services |
| Delivery | Git-based CI/CD with policy checks and signed build artefacts |
| Data | Managed relational stores for transactional systems, object storage, plus warehouse or lakehouse patterns for analytics |
| Observability | Metrics, logs, tracing, alerting, and audit event pipelines |
| Integration | API gateway, event bus, and standard adapters for legacy systems |
The exact vendor mix will vary. Some organisations keep more on-premise components because of procurement, latency, or residency constraints. Others lean heavily on managed services to reduce operational burden. The important point is to choose a stack that the platform team can operate consistently.
How AI Changes the Architecture
AI-enabled healthcare platforms need more than a model endpoint. According to this guidance on platform engineering for AI in healthcare, security, transparency, encryption, vulnerability management, and audit logging must be built into every workflow from day one, with a shared evaluation infrastructure to compare model behaviour consistently.
That requirement changes the reference architecture in two ways.
First, model development and model serving need shared control points. Teams should use common pipelines for artefact registration, approval, deployment, and monitoring rather than shipping models as bespoke application features.
Second, evaluation has to be platformised. If each team measures model quality, drift, and operational behaviour differently, governance becomes uneven, and comparisons become meaningless.
The safest place to enforce AI controls isn't inside each product team's custom code. It's in the platform services every team already depends on.
Buy, Build, and Hybrid Decisions
Most healthcare organisations shouldn't build everything. Identity, secrets management, managed databases, and baseline monitoring are usually better consumed than invented. But the internal developer platform itself often needs custom assembly because it reflects local governance, local workflows, and local integration realities.
That's where the architecture discipline matters. Build the opinionated layer that encodes your standards. Buy the undifferentiated services that mature vendors can run better than you can.
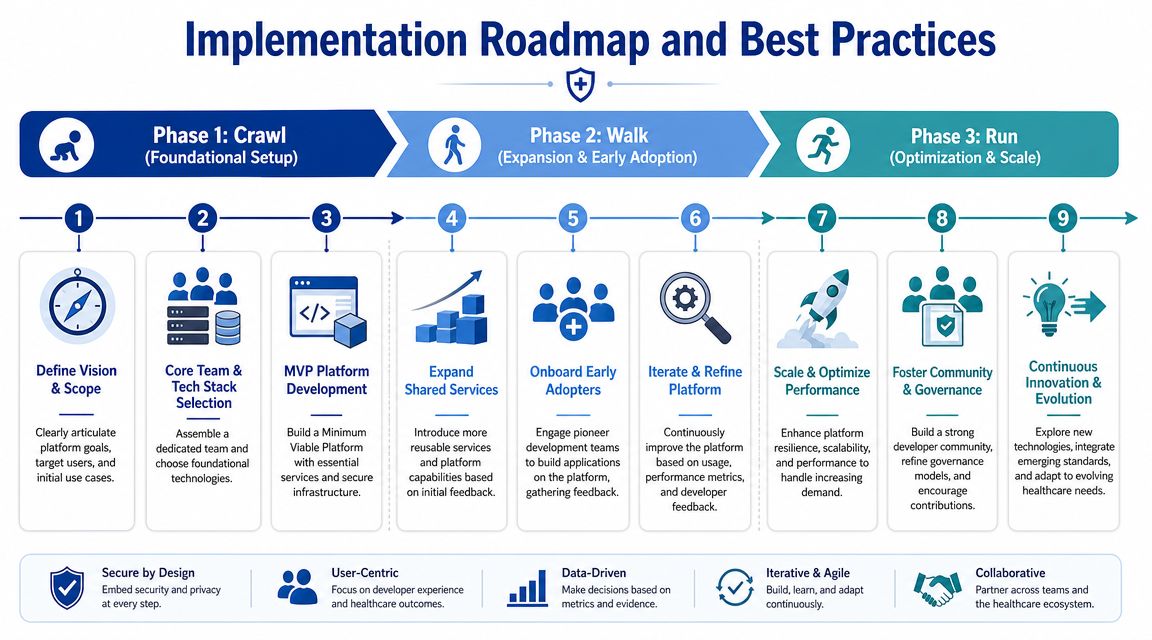
Implementation Roadmap and Best Practices
The biggest implementation mistake is trying to launch a complete enterprise platform in one motion. That usually produces a large, abstract programme with weak adoption. A better approach is phased, product-oriented, and tied to real delivery teams.

Crawl
Start with one golden path for one team and one class of workload. Pick a product that matters but won't collapse the programme if something needs redesign. Build only the minimum platform features required to make that team faster and safer.
That usually includes:
A standard deployment template: Container build, environment promotion, secrets, and rollback.
Baseline security controls: Identity integration, encryption defaults, and audit logging.
Core observability: Logs, metrics, traces, and alert routing that work out of the box.
A lot of teams benefit from practical Infrastructure as Code guidance at this stage. This resource for DevOps teams on Terraform is useful because it focuses on how teams standardise infrastructure changes rather than treating provisioning as ad hoc operations.
Walk
Once one team is shipping successfully, expand services based on observed friction. Don't add features because they look complete on an architecture slide. Add them because the second and third teams need them.
Typical additions include a service catalogue, reusable API templates, integration accelerators, central policy checks, and curated data access workflows. This is also a good point to formalise product management for the platform. Someone must own adoption, support, prioritisation, and documentation.
An organisation that wants to systematise provisioning and release patterns can use models such as platform engineering with Infrastructure as Code to shape those internal services. Cleffex Digital Ltd is one example of a firm that builds software for regulated healthcare workflows, which is relevant when teams need implementation support rather than just conceptual guidance.
Run
At the mature stage, the platform becomes a true internal product. Teams can self-serve approved capabilities, request exceptions through defined channels, and rely on published service levels. Governance becomes more predictable because the default path is already aligned to policy.
A mature platform also has to address equity and access. California's experience highlights a challenge that applies far beyond one state: platform benefits must reach under-resourced clinics and diverse populations, not only large health systems, as discussed in this piece on AI and underserved communities in healthcare. For Canadian organisations, that means designing for smaller providers, varied digital maturity, language needs, and constrained operational capacity.
Best Practices That Hold Up in Real Delivery
Treat the platform as a product: It needs a roadmap, user research, documentation, and support.
Optimise for developer behaviour: If the paved path is slower than local improvisation, teams will bypass it.
Make governance visible: Publish standards, exception processes, and ownership boundaries clearly.
Design for small teams too: A platform that only works for large centralised engineering groups won't improve the broader care ecosystem.
Measuring Success and Avoiding Common Pitfalls
A healthcare platform should be measured from two directions. One is team effectiveness. The other is operational confidence. If you track only adoption, you'll miss whether the platform improves delivery. If you track only control coverage, you'll miss whether teams are avoiding it.
Useful measures are usually qualitative and operationally grounded: how long it takes a team to get a new service into a compliant environment, how often releases require manual intervention, whether incidents are easier to investigate, whether access requests are clearer, and whether internal reviews spend less time on repeated baseline issues.
What Good Progress Looks Like
Developers use the paved path voluntarily: The platform saves them time.
Security reviews focus on exceptions: Baseline controls are already inherited.
Operations sees more consistency: Services expose standard telemetry and support patterns.
Leaders get cleaner risk signals: They can tell which systems follow approved patterns.
Common Failure Modes
The most expensive mistakes are familiar. Platform teams build for architectural purity instead of developer needs. Governance groups add process but not usable automation. Leadership funds an initial build, but not long-term product ownership. Teams promise self-service while hiding approvals behind tickets and manual reviews.
If engineers need a platform team meeting to complete normal work, the platform isn't self-service yet.
Healthcare platform engineering matters because it turns a scattered technology estate into an operating model. In Canada, where regulation, fragmentation, and data sensitivity intersect every day, that isn't a nice-to-have. It's how modern digital health systems stay shippable, governable, and supportable.
Cleffex Digital Ltd helps organisations build secure, scalable software systems for regulated environments, including healthcare. If you're planning a healthcare platform engineering initiative and need support with architecture, cloud foundations, AI-enabled workflows, or compliant product delivery, explore Cleffex Digital Ltd.







