



A patient sees a family physician in one system, gets bloodwork through a separate lab network, visits a hospital that stores results elsewhere, and then follows up with a specialist using another portal. By the time the care team tries to build a complete picture, staff are logging into multiple systems, re-entering data, chasing faxed records, and guessing whether the medication list is current.
That situation isn't just irritating. It adds operational drag to every clinical workflow and increases risk at the exact moment the organisation is trying to improve access, patient experience, and reporting. Canadian healthcare leaders already know the problem. What they often need is a practical path out of it.
FHIR integration services matter because they turn interoperability from a standards discussion into an implementation programme. The actual work isn't learning the acronym. It's deciding how to connect legacy systems, where to place the API layer, how to secure PHI, and how to get measurable value without breaking the workflows staff depend on today.
The High Cost of Disconnected Health Data
Disconnected health data appears first in patient journeys, not in architecture diagrams. A patient arrives at an urgent visit after seeing multiple providers in the past month. The clinician can see part of the history in the local EHR, but not the specialist note, not the latest lab result, and not the medication update made elsewhere. Staff starts making phone calls. Someone prints a summary. Someone else re-types data into another screen.
That delay has a business cost as well as a clinical one. Teams spend time reconciling records instead of delivering care. Duplicate testing becomes more likely. Front-line staff lose confidence in what they're seeing because each application presents only a partial record.
Where the Cost Actually Lands
For CIOs and programme managers, the damage usually appears in four places:
Operational overhead: Integration teams maintain brittle point-to-point interfaces that are hard to reuse and expensive to change.
Clinical friction: Clinicians work around missing data by calling, faxing, or repeating intake questions.
Digital product delays: Patient portals, mobile apps, and analytics initiatives stall because each new use case needs another custom connection.
Governance strain: Privacy, consent, audit, and access controls become harder when data moves through inconsistent channels.
Disconnected systems don't fail all at once. They fail one workflow at a time.
In Canada, this problem is amplified by regional variation. Hospitals, clinics, provincial programmes, and third-party applications often need to exchange information across organisational boundaries, while still fitting local workflow and policy constraints. A custom integration approach might solve one project, but it usually creates more maintenance work for the next one.
Why FHIR Is the Practical Answer
FHIR integration services thus become strategic. They give organisations a standard way to expose and consume health data through APIs, rather than building a new one-off interface for every partner, portal, or product. That shift changes the economics of interoperability.
Instead of asking, “How do we connect System A to System B?” the better question becomes, “What reusable integration pattern should we establish so the next five systems are easier to onboard?” That's the point at which interoperability stops being an IT burden and starts becoming infrastructure.
Understanding FHIR Integration Services
FHIR is best understood as a universal translator for healthcare data. Different systems still store data in different ways, but FHIR gives them a common structure and API style for exchanging it. That's why it has become central to modern interoperability work.
According to healthit.gov's overview of FHIR, FHIR was created by HL7 as an API-focused standard for quickly and efficiently exchanging clinical and administrative health data. The same source also notes that it provides a common data model and RESTful API layer for connecting EHRs, patient portals, labs, and mobile apps. In the Canadian context, that matters because interoperability programmes have moved from discussion to implementation, with standardised exchange becoming more useful than custom point-to-point interfaces.
The Standard Is Not the Service
This distinction matters in procurement conversations. FHIR itself is the standard. FHIR integration services are the implementation layer that makes the standard useful in your environment.
A service partner typically handles the work that the standard alone doesn't solve:
API design: Defining which resources, endpoints, and operations your systems will expose.
Transformation logic: Mapping existing records into FHIR resources in a way that fits actual workflows.
Security controls: Applying authentication, authorisation, audit, and access management around PHI.
Operational reliability: Handling retries, errors, throttling, monitoring, and version control.
Without that layer, organisations often discover they have “FHIR support” in theory but no dependable way to use it in production.
Why Canadian Organisations Should Care
Canadian healthcare buyers usually aren't asking what FHIR is anymore. They're asking whether it can help them connect an EHR, a provincial repository, a patient app, and a reporting system without multiplying interface debt. That is the right question.
FHIR integration services create value when they support a broader operating model:
| Need | What FHIR integration services add |
|---|---|
| Patient-facing digital services | A cleaner API layer for portals and mobile apps |
| Cross-system exchange | Reusable patterns instead of one-off interfaces |
| Vendor ecosystem growth | A standard entry point for new applications |
| Analytics readiness | Cleaner, more consistent data access across systems |
Teams exploring automation often face a related challenge outside the clinical stack as well. If you're also reviewing integrations for managing AI employees, the lesson is similar. Standards and connectors only create value when they fit the operating model, governance rules, and day-to-day workflows of the organisation using them.
Practical rule: Buy FHIR integration services for workflow outcomes, not for API availability alone.
Key Offerings From an Integration Partner
A credible FHIR integration partner doesn't just stand up endpoints and call the job done. The work spans architecture, data modelling, security, workflow design, and long-term operability. If a vendor proposal focuses only on “FHIR API development,” it's usually too narrow.
Hybrid Integration, Not Forced Replacement
One of the most common misconceptions is that adopting FHIR means replacing HL7 v2 immediately. In practice, it usually doesn't. A 2023 review on barriers to FHIR adoption described issues such as variation in EHR implementation, limited vendor support, ontology variation, workforce knowledge gaps, and testing limitations. That's why many organisations need a hybrid model where FHIR sits beside legacy HL7 and document-based exchange rather than replacing them overnight.
That point is especially relevant in Canada. Ontario's Digital Health Drug Repository already uses FHIR for some access patterns, yet broader provincial interoperability still has to coexist with older integration methods. Buyers should treat migration architecture as a first-class requirement, not a future clean-up task.
What a Complete Service Should Include
The strongest partners usually cover the following layers.
Legacy data mapping: They map HL7 v2 messages, proprietary schemas, and administrative records into FHIR resources that make sense for your environment.
Middleware or orchestration: They build or configure the integration layer that routes, transforms, validates, and monitors transactions.
Security implementation: They apply OAuth 2.0, token handling, access controls, logging, and audit patterns around every exchange path.
Testing discipline: They don't wait until go-live to discover that a resource profile or workflow assumption was wrong.
Operational handover: They define who owns support, versioning, endpoint changes, and exception management after launch.
What Buyers Should Ask for in Detail
A useful vendor evaluation goes deeper than product brochures. Ask specific questions such as:
| Area | Good sign | Warning sign |
|---|---|---|
| Legacy coexistence | Clear plan for HL7 v2, documents, and phased migration | “We'll convert everything to FHIR later” |
| Clinical workflow fit | Mapping decisions tied to real user journeys | Technical design with no user validation |
| Consent and audit | Explicit controls for access, traceability, and exceptions | Privacy treated as a post-build task |
| Production support | Monitoring, rollback, and incident ownership defined | Support model is vague |
Some organisations also need a development partner that can bridge healthcare integration with broader software delivery. For example, Cleffex Digital Ltd provides healthcare software integration work that includes EHR and HL7 FHIR integration, which can be relevant when an organisation needs both interoperability engineering and custom application delivery in the same programme.
What Tends Not To Work
The failed projects usually share a pattern. The team starts with a technical standard, not a business use case. They expose resources no application needs, ignore source data quality, and postpone governance until after the build. Then production users discover that the integration is technically valid but operationally awkward.
If the partner can't explain how a medication update, referral, or lab result moves through your workflow, they're not ready for your project.
Choosing Your FHIR Architecture Pattern
Architecture decisions shape cost, speed, and long-term flexibility more than the first API sprint ever will. Most Canadian organisations end up choosing between a few common patterns, each with different trade-offs for PHI handling, performance, and operational control.
A useful way to frame the decision is this: do you want FHIR to act mainly as an access layer, as a central data hub, or as a set of specialised services around a broader platform?
Pattern Comparison
Canadian healthcare interoperability is increasingly shaped by cloud and API deployment models. Microsoft describes its Azure API for FHIR overview as a managed FHIR-compliant server that can be provisioned in minutes, with an enterprise-grade RESTful API endpoint for storing, ingesting, and querying FHIR data. That kind of managed service is attractive when regional health systems and vendors need secure handling of protected health information across multiple applications and care settings.
The architecture still needs to match the organisation.
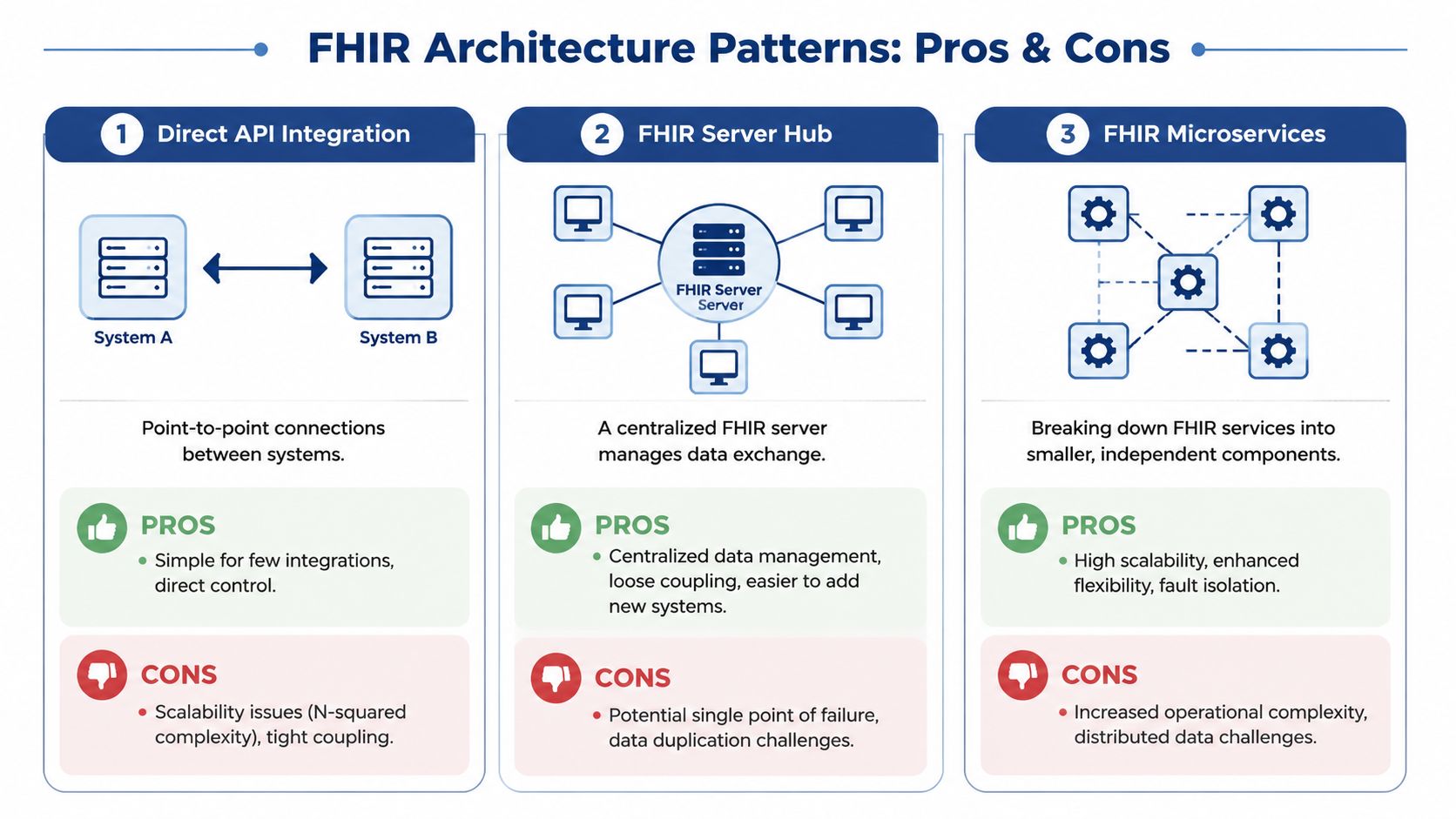
| Pattern | Best for | Strengths | Trade-offs |
|---|---|---|---|
| Direct API integration | Small scope, few systems | Fast to start, low initial complexity | Tight coupling, hard to scale |
| FHIR server hub | Regional exchange, patient apps, analytics | Central governance, reusable integration surface | Data duplication and hub dependency |
| FHIR microservices | Large programmes with multiple digital products | Flexibility, domain-specific scaling | Higher operational complexity |
When Each Pattern Makes Sense
Direct API Integration
This works when the organisation has a narrow use case and a limited number of source systems. A clinic exposing demographics and basic observations to a patient application may get value quickly from a direct pattern.
The problem appears later. Every new connection becomes another custom dependency. Over time, the architecture starts to look like the same interface sprawl FHIR was supposed to reduce.
FHIR Server Hub
This is often the most practical middle ground for Canadian providers and digital health vendors. A central FHIR server can act as the standard exchange point for portals, mobile apps, and selected clinical systems.
It's also a good fit when leadership wants consistent API governance, standard search behaviour, and cleaner onboarding for future applications. If your team is reviewing broader enterprise application architecture patterns, this hub model usually maps well to organisations that need both interoperability and platform reuse.
FHIR Microservices
This pattern fits mature engineering teams supporting multiple products or care domains. One service may focus on patient identity, another on observations, another on scheduling or consent workflows.
It offers flexibility, but it also raises the bar for operations. Teams need stronger service governance, observability, release discipline, and cross-service data management. For many healthcare organisations, that's a target state, not a starting point.
The Decision Rule That Helps
Choose the simplest pattern that supports the next several use cases, not just the first one. That usually leads smaller programmes toward a hub or facade approach rather than direct point integrations that will need redesign later.
Your Phased FHIR Implementation Roadmap
Most FHIR projects fail when teams treat implementation as a connector build instead of a controlled transformation programme. The safest path is phased, with clear gates for mapping, validation, security, and workflow fit.
For Canada-specific deployments, implementation guidance highlighted by Aniso Solutions on FHIR API integration in healthcare identifies the primary constraint: not FHIR syntax, but conformance and workflow mapping. That means mapping legacy records into standardised resources, choosing a version such as R4, defining endpoints and error-handling patterns, applying OAuth 2.0 and SMART on FHIR, and running conformance tests before production.
Phase 1 and 2: Define Whether the Project Stays Under Control
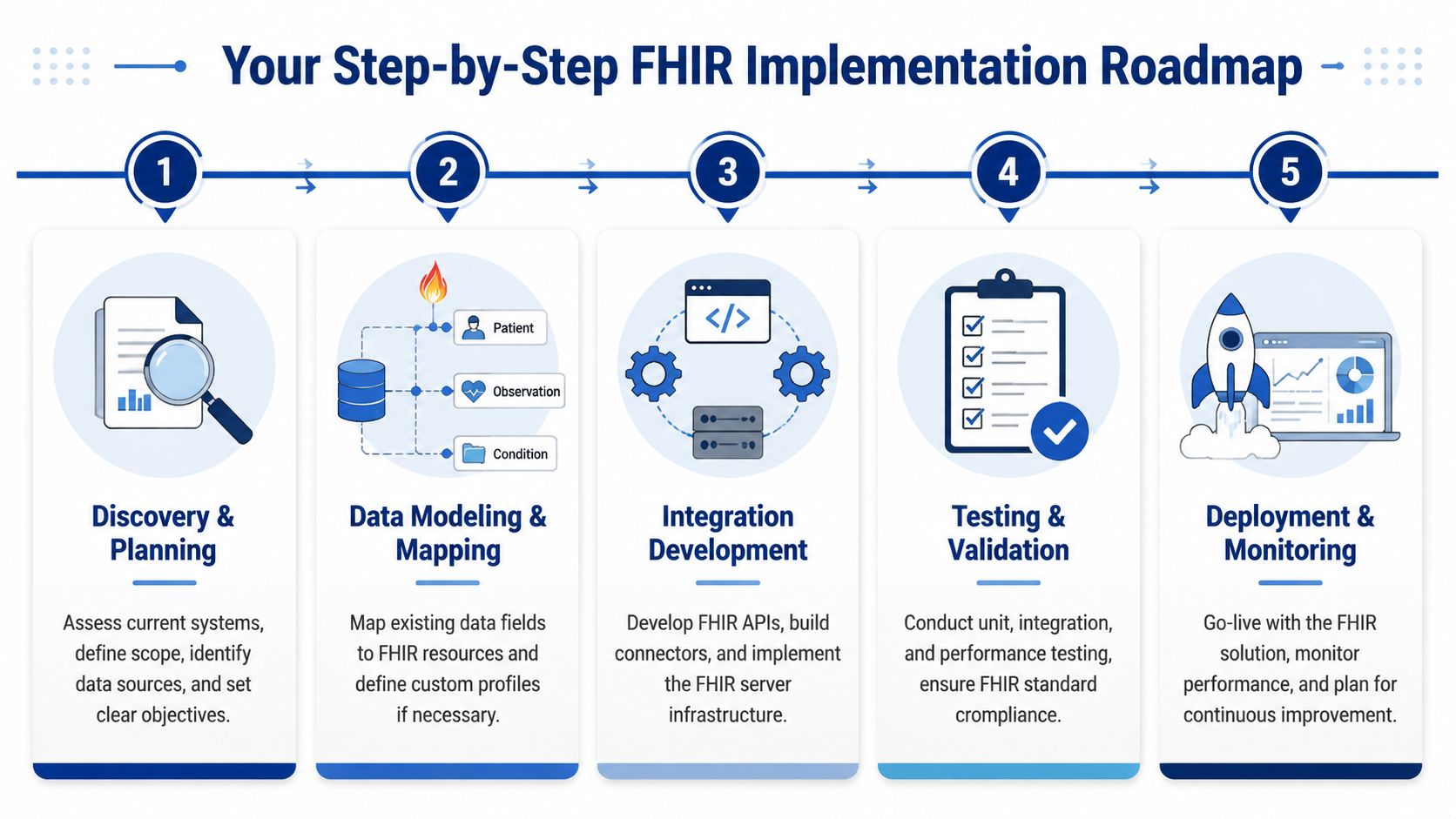
Discovery and Planning
Start with business priorities, not resource lists. Decide which workflows need improvement first. Common starting points include patient access, lab result exchange, referral workflows, or selected data feeds for analytics.
Then identify system owners, data stewards, privacy stakeholders, and operational support leads. If those groups don't agree on scope and ownership early, technical progress won't save the project later.
Data Modelling and Mapping
Nevertheless, optimism often gets tested. Source systems rarely map cleanly to standard resources. Fields are overloaded, codes are inconsistent, and workflows vary by site.
Use a mapping catalogue. Define what comes from where, how it transforms, which profile it targets, and how exceptions are handled. A practical reference for technical teams planning this work is Cleffex's guide to integrating FHIR with EHR systems, especially when the challenge includes both legacy EHR access and standards-based exchange.
Phase 3 and 4 Separate Demos From Production Systems
Integration development: Build the API layer, transformation rules, authentication, and audit controls. Make error handling explicit. Silent failure is dangerous in healthcare workflows.
Testing and validation: Run unit tests, workflow tests, conformance checks, and realistic scenario validation with actual users. Don't stop at schema validation.
A resource can be technically valid and still be wrong for the care process it's meant to support.
Two testing mistakes come up often. First, teams validate isolated resources but not cross-system workflows. Second, they test with ideal data rather than the messy records that production holds.
Phase 5 Turns Implementation Into an Operating Capability
Deployment and monitoring
Go live in controlled increments. Start with a limited set of consumers or a contained workflow. Watch audit logs, error rates, token behaviour, and user support tickets closely.
After launch, keep a backlog for optimisation. You'll almost always need adjustments to mapping, search behaviour, terminology handling, or operational dashboards once real usage begins.
What Drives Timeline and Cost
The biggest drivers are usually qualitative rather than mathematical:
Legacy complexity: Older systems with inconsistent data structures take more mapping effort.
Workflow variation: The same “lab result” process may behave differently by site or partner.
Governance maturity: Decisions move faster when ownership, privacy review, and release control are already organised.
Data quality: Bad identifiers and inconsistent coding create rework throughout the build.
The teams that move fastest are not the ones writing code first. They're the ones that lock down scope, ownership, and conformance discipline before the first production endpoint appears.
Real-World Use Cases and Measurable ROI
Business value from FHIR integration services doesn't come from the standard itself. It comes from reducing manual coordination, improving access to usable data, and making new services easier to launch without rebuilding the integration layer each time.
Three Practical Examples
A community clinic network often starts with patient access. Staff want one portal view that pulls demographics, appointments, medications, and lab summaries from different systems. The ROI shows up in fewer manual record requests, less front-desk follow-up, and a better digital experience for patients who no longer need to chase their own information.
A hospital programme may focus on clinician workflow instead. A FHIR layer can support near real-time access to observations, medication information, and encounter context across connected applications. That doesn't just help with visibility. It gives digital teams a reusable way to support decision support tools, patient-facing modules, and downstream reporting without rebuilding each time.
A regional or public-health-oriented initiative may use FHIR to aggregate data for population-level views across multiple organisations. The value here is governance and reuse. Once a standard exchange pattern exists, onboarding additional participating systems becomes more manageable than maintaining unique connections for each pair of organisations.
Social Needs and Reimbursement Are Becoming More Relevant
A less discussed use case is non-clinical data. A Unite Us report on FHIR integration notes that FHIR is increasingly being used to share screening data for drivers of health, such as housing and food insecurity, while also helping streamline reimbursement through standardised non-medical screenings and interventions.
That matters in Canada because broader patient-centred care often depends on linking community services with healthcare delivery. The technical challenge isn't just exposing a FHIR endpoint. It's deciding how social-needs data maps into clinical and administrative systems, how consent works, and how funding or reimbursement logic is represented in the workflow.
What ROI Looks Like in Practice
The most defensible returns tend to appear in these areas:
Lower integration overhead: Teams reuse API and mapping patterns instead of building every connection from scratch.
Faster digital delivery: Patient apps, provider tools, and reporting services can launch against a standard access layer.
Reduced administrative friction: Staff spend less time gathering and re-entering information across systems.
Better data availability for planning: Organisations gain a cleaner foundation for analytics and cross-setting reporting.
ROI is strongest when the project starts with one expensive workflow problem and builds outward from there.
Selecting a Partner and Ensuring Compliance
Vendor selection in healthcare should be sceptical by design. A polished FHIR demo doesn't prove a partner can manage legacy coexistence, privacy controls, production support, or workflow complexity in a Canadian environment.
The Shortlist Questions That Matter
Ask potential partners these questions before you review pricing in detail:
How do you handle hybrid environments? You want a concrete coexistence strategy for FHIR, HL7 v2, documents, and proprietary source systems.
How do you support privacy by design? In Canada, that includes careful treatment of PIPEDA obligations alongside local health information rules and organisational policy.
How do you validate workflow fit? The answer should include clinicians, operations staff, and realistic scenario testing.
How do you manage security operations? Look for auditability, least-privilege access, encryption, incident handling, and clear ownership after go-live.
If your internal team needs a stronger baseline on security governance, this guide to the ISMS standards ISO 27001 is a useful reference for evaluating whether a partner's controls are mature enough for regulated environments.
Compliance Is Architecture, Not Paperwork
PIPEDA compliance doesn't sit at the end of the project. It affects data minimisation, consent handling, retention, audit logs, access control, and vendor responsibilities from the start. The same is true for broader secure development practice. Teams comparing suppliers should look at how they approach compliance-driven software development rather than accepting a generic assurance statement.
Choose the partner that can explain your exceptions, not just your happy path.
A strong integration partner acts like an implementation guide, not a code factory. They should be able to tell you what not to connect yet, what should remain hybrid for now, and where governance needs to tighten before scale makes problems harder to fix.
If your organisation is planning a FHIR programme and needs help with architecture, phased delivery, or secure healthcare integration, Cleffex Digital Ltd can support discovery, custom software delivery, and interoperability implementation work in a Canadian context.







