



USD 7.08 billion in 2024, projected to reach USD 13.16 billion by 2035 at a 5.8% CAGR from 2025 to 2035. That's the current scale and projected growth of the Healthcare Enterprise Software Market, according to Market Research Future. For anyone planning enterprise healthtech platform development, that number changes the conversation.
This isn't about shipping another patient app or dashboard. In Canada, the hard part isn't feature development. It's building a platform that can survive procurement, integrate with fragmented provincial systems, satisfy privacy expectations, and still give operations teams something they can use.
The first platform usually fails for predictable reasons. Teams overbuild before they validate workflows. They treat interoperability as a later phase. They confuse FHIR support with integration readiness. They write compliance policies, but don't implement controls. The result is expensive software that works in a demo and struggles in a hospital environment.
A workable Canadian approach is narrower and more disciplined. Start with real workflows. Build for multi-jurisdiction integration from day one. Use standards where they help, but don't assume standards remove migration work. Make security observable, not just documented. If AI is part of the roadmap, treat governance as product functionality.
What Is an Enterprise Healthtech Platform
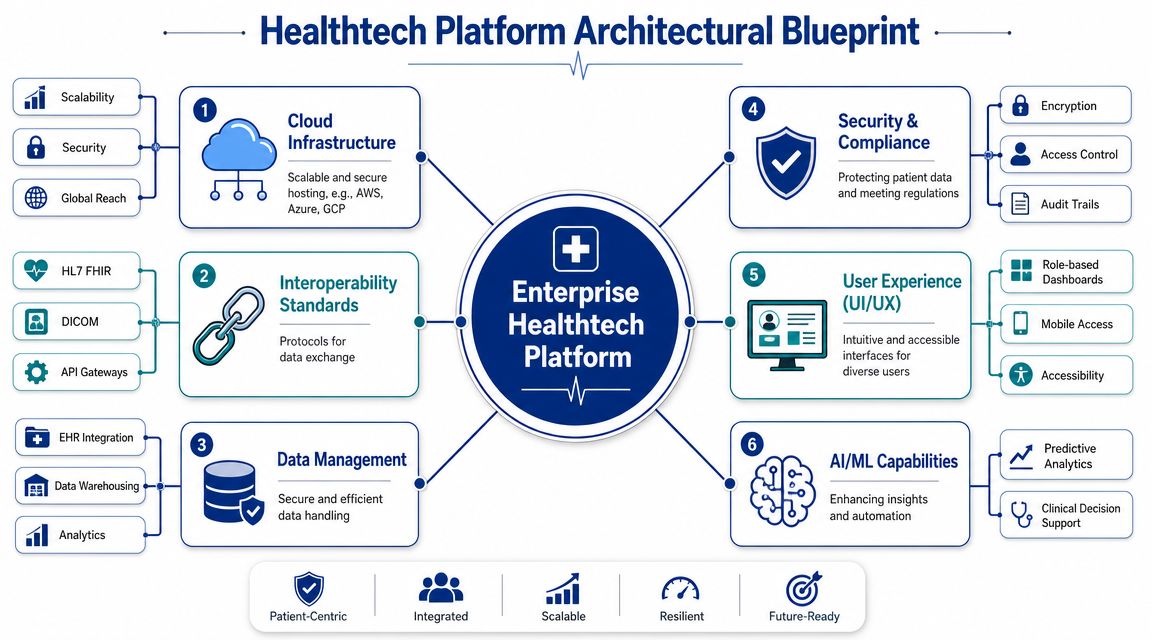
An enterprise healthtech platform is the digital backbone that connects clinical, operational, and administrative systems across a healthcare organisation. It isn't just an EHR add-on, a patient portal, or a billing tool. It's the layer that lets those systems exchange data, enforce rules, and support workflows without forcing staff to re-enter the same information in five places.
That distinction matters because healthcare organisations rarely operate from one clean system. They run a mix of EHRs, scheduling tools, referral workflows, telehealth products, billing platforms, identity systems, document repositories, and analytics layers. Without a unifying platform, each integration becomes a one-off project. Maintenance costs rise. Data quality drops. Teams lose trust in the system.

What the Platform Actually Does
A good platform acts like a digital nervous system for the organisation. It receives signals from multiple systems, normalises them, routes them to the right destination, and records what happened.
In practical terms, that usually includes:
Integration services that connect EHRs, labs, imaging, billing, CRM, and patient-facing applications
Identity and access layers that control who can view, change, or export information
Workflow orchestration for referrals, intake, triage, discharge, follow-up, and internal approvals
Audit and security controls that make enterprise procurement possible
Shared data services that support reporting, analytics, and eventually AI
If a clinic group wants to automate healthcare intake and booking, for example, the platform should connect intake forms, patient identity, appointment availability, notifications, and downstream records. Without that shared foundation, automation usually stops at the front door.
Practical rule: If your “platform” only serves one department and doesn't simplify cross-system workflows, it's probably an application, not a platform.
What Makes It Enterprise-Grade
Enterprise healthtech platform development is less about visual polish and more about operational discipline. Enterprise buyers expect the system to be reliable under stress, traceable during audits, and adaptable when another hospital, clinic, or province enters the picture.
That changes architecture decisions early. A startup can get away with manual reconciliation and brittle integrations for a while. A health authority or multi-clinic network can't. They need a platform that supports standardised processes without erasing local variation.
The strongest platforms don't try to replace every existing tool. They reduce fragmentation by making those tools work together under shared governance.
Defining Your Business and Clinical Requirements
Most platform failures start before engineering. The team picks a stack, drafts a roadmap, and only later asks which workflows matter most. In healthcare, that order causes damage fast because technology choices are consequences of workflow choices, not the starting point.
Take a multi-clinic practice expanding into new regions. Leadership might say they need “one platform” for scheduling, referrals, patient engagement, and reporting. That statement is too broad to build from. You need to identify who uses the system, what decision each user is trying to make, and where current handoffs break.
Start With Users Who Carry Operational Risk
In a typical multi-clinic setup, four groups shape requirements more than anyone else:
Clinicians need the fewest clicks possible between review, documentation, and follow-up.
Front-desk and intake staff need reliable identity matching, appointment rules, and exception handling.
Clinic managers need visibility into throughput, no-shows, pending referrals, and staffing bottlenecks.
Patients need simple access points that don't create more inbound support work.
Notice what's missing. “Admin dashboard” isn't a requirement. “AI assistant” isn't a requirement. Those may become features later. The requirement is that the job needs to be completed safely and consistently.
Map Workflows Before Features
A strong requirements process looks at a handful of critical workflows in detail. Don't map everything. Map the workflows that create the most rework, delay, compliance risk, or revenue leakage.
For a growing clinic network, those usually include:
New Patient Intake
Where does demographic data enter? Who verifies consent? How is duplicate identity handled? What happens when the patient books online but arrives with different information?Referral Processing
How does the referral arrive? Fax, portal, direct message, manual upload? Who triages it? What rules determine urgency, speciality, and booking destination?Results and Follow-Up
Which events trigger outreach? Who owns unresolved items? How are patient communications logged?Cross-Clinic Scheduling
Can one site view another site's capacity? What exceptions require manual approval? How are reschedules handled when the source system differs by location?
A platform requirement should be written in terms of behaviour, controls, and outcomes. “The system must support referrals” is vague. “The system must ingest referrals from multiple channels, route them by clinic rules, assign ownership, and preserve an audit trail” is useful.
The fastest way to bloat a platform is to collect feature requests without ranking the workflows they support.
Separate Must-Haves From Future Leverage
Teams often mix launch requirements with strategic ambitions. That creates oversized MVPs and long delays. I'd separate requirements into three bands.
| Requirement band | What belongs here | Typical examples |
|---|---|---|
| Non-negotiable at launch | Items tied to safety, compliance, billing, or core operations | patient identity, access controls, auditability, intake, scheduling, referral routing |
| Needed for adoption | Features that reduce friction for daily users | mobile-friendly staff screens, templated communications, and role-based dashboards |
| Later leverage | Valuable once the data foundation is stable | advanced analytics, AI summarisation, population risk views |
This prioritisation makes trade-offs visible. If the budget is tight, you don't cut auditability to fund a polished portal. You defer less impactful features and protect the core workflow spine.
Requirements quality improves when product, operations, clinical users, and compliance all review the same workflow maps. That shared view usually reveals the underlying issue. It's often not “we need more software.” It's “handoffs are unowned, data is inconsistent, and nobody trusts the current process.”
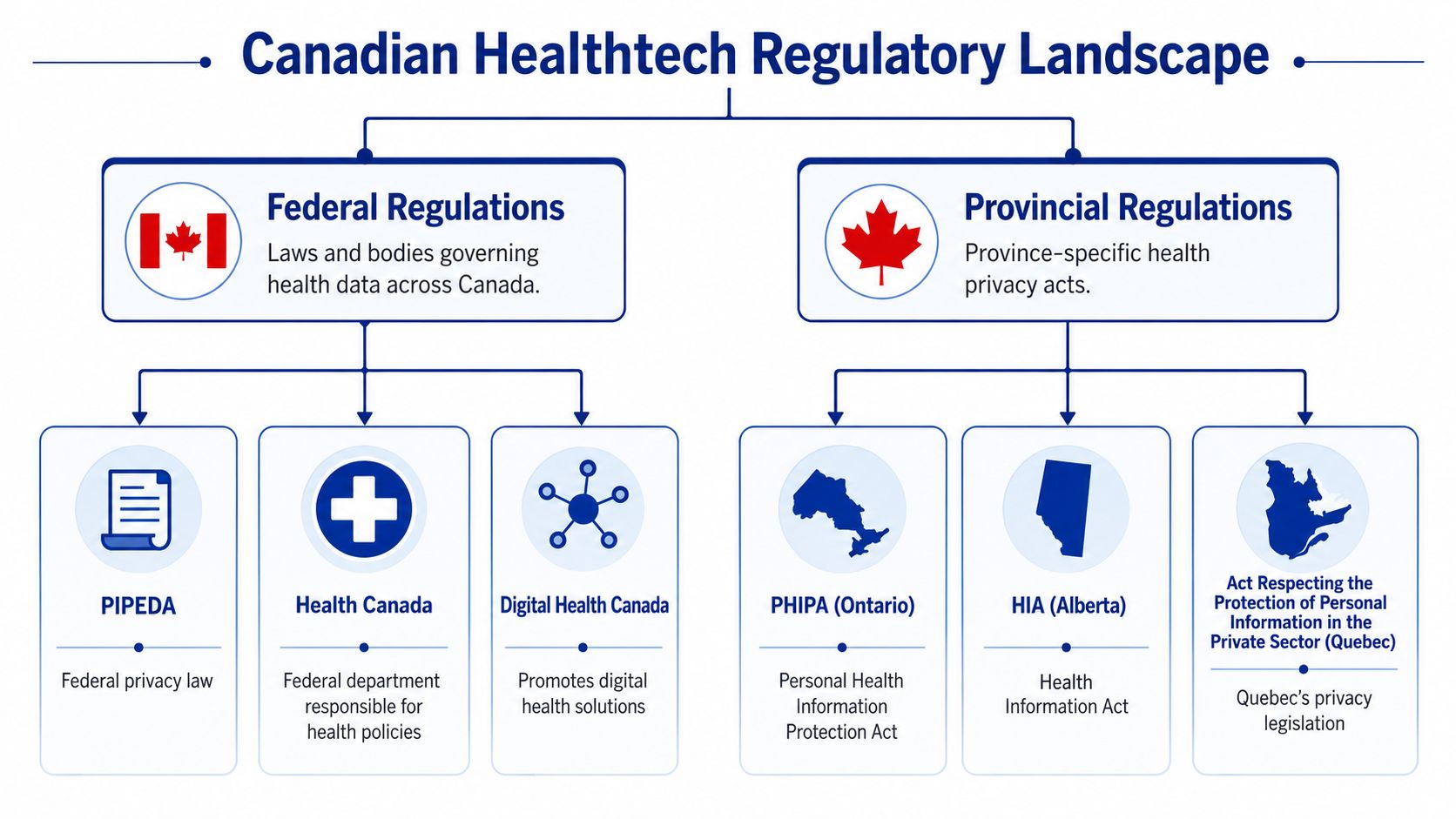
Navigating the Canadian Regulatory Maze
Canadian healthtech teams get into trouble when they treat regulation as a document exercise. Policies matter, but enterprise buyers don't purchase policies. They evaluate whether your platform enforces controls in production.
That's why compliance should be treated as architecture. The Office of the Privacy Commissioner of Canada emphasises safeguards appropriate to the sensitivity of personal information. In practical platform terms, that means building role-based access control, immutable audit logging, and encryption in transit and at rest into the system itself, as described in this discussion of Canadian privacy-by-design controls.
Build Controls Where Access Actually Happens
Many teams write access rules in a policy binder and then implement permissive application logic because it's faster. That doesn't hold up under enterprise review. Access decisions need to be enforced at the API gateway and service layer, where data is requested and returned.
A workable baseline includes:
Role-based access control tied to real job functions, not generic labels
Immutable audit logs that can reconstruct who accessed which record, when, and from where
Encryption in transit and at rest across production systems and stored data
Retention and disposal controls are aligned with the sensitivity of health information
Environment segregation so development shortcuts don't leak into production risk
For organisations evaluating AI-specific obligations, this paper on Developing compliant healthtech AI platforms is useful because it frames compliance as a design problem, not a legal add-on.
Privacy-by-Design Shortens Sales Cycles
A lot of founders assume compliance slows growth. In enterprise healthtech, weak compliance slows growth much more. Procurement teams ask detailed questions about access reviews, incident handling, auditability, data segregation, and vendor responsibility. If your answers rely on manual workarounds, the deal drags.
That's why privacy-by-design has commercial value. It gives buyers evidence that your platform won't create unnecessary operational risk after go-live.
If you need a broader view of how regulated workflows affect engineering decisions, this guide to healthcare compliance software development is a helpful reference point.
Architecture check: If support staff can't answer “who saw this record?” from system evidence, you don't have enterprise-grade auditability.
Canadian Reality Is Layered, Not Uniform
The phrase “Canadian compliance” can be misleading. Buyers operate across federal and provincial expectations, and some organisations also need HIPAA-adjacent controls for cross-border relationships. That doesn't mean you should build for every jurisdiction at once. It means your platform should support policy variation without changing core architecture.
The cleanest way to do that is to separate control mechanisms from policy settings. Keep the enforcement primitives stable. Then configure retention, disclosure, consent, and workflow rules by customer or jurisdiction as needed.
That structure works better than hardcoding local assumptions into every module. It also keeps your system maintainable when the product expands to another province or another class of enterprise buyer.
Architecting for Interoperability and Scale
Interoperability is where Canadian platform plans become real or fall apart. Teams say they support FHIR, but what they often mean is they can read or produce a few standard resources. That's not enough for enterprise healthtech platform development in a federated system.
Canada's practical challenge is uneven maturity across provinces, hospitals, labs, and vendors. Some environments expose modern APIs. Others still depend on older HL7 patterns, batch extracts, custom files, or manual workarounds. The winning architecture doesn't assume a clean standardised world. It creates order in a messy one.
Treat FHIR as an API layer
The most useful technical stance is to treat HL7 FHIR as an API layer, not just a document format. That means you normalise core entities such as Patient, Encounter, Medication, and Observation into a canonical model, then map vendor-specific or province-specific schemas into that model through adapters, as outlined in this piece on scaling securely with healthtech integrations.
This design gives you three advantages:
Connector reuse because business logic isn't tied directly to each source system
Cleaner analytics because downstream reporting reads from a vendor-neutral model
Lower integration debt when you add new hospitals, labs, or referral sources
It also makes migration survivable. Legacy systems rarely disappear on your timeline. A canonical model lets the new platform coexist with old workflows while you retire brittle interfaces in stages.
Why FHIR Compatibility Still Fails in Practice
A platform can be technically FHIR-compatible and still fail operationally. Common reasons include poor identity resolution, inconsistent coding, event timing mismatches, and weak governance around API changes.
The core work usually sits in four areas:
| Layer | What teams often underestimate | What works better |
|---|---|---|
| Identity | Assuming patient identifiers align across systems | Introduce deterministic and reviewed matching rules |
| Data semantics | Treating field mapping as enough | Normalise concepts and document value-set translation |
| Workflow timing | Expecting source systems to publish clean, real-time events | Design for async updates, retries, and reconciliation |
| API governance | Letting each integration evolve independently | Version interfaces and document contracts centrally |
If your team wants better discipline around interface definitions, OpenAPI tooling and workflows can help standardise contract design and documentation for the services around your canonical model.
“FHIR support” answers a procurement checkbox. It doesn't answer how your platform handles duplicate patients, partial records, or delayed lab feeds.
Choose Architecture Based on Change Patterns
The cloud, service boundaries, and deployment model should match how the platform will change. Don't default to microservices because the system is “enterprise.” Many first platforms are better served by a modular monolith with strict boundaries, especially when the team is small and domain rules are still changing.
I'd use this rule set:
Choose a modular monolith first when workflows are still being discovered, and the team needs fast iteration.
Split services deliberately when domains have distinct scaling, security, or release needs.
Keep integration adapters isolated so source-specific changes don't ripple into core workflow logic.
Create one audited platform gateway instead of exposing ad hoc service endpoints to every client and partner.
For broader patterns around integrated care systems, this article on connected healthcare platforms gives a useful systems-level view.
Scale Comes From Boring Foundations
Teams often think scale means Kubernetes, event streams everywhere, and a long vendor shortlist. In healthtech, scale usually comes from less glamorous choices. Stable APIs. Clear ownership. Observability. Retry logic. Queue handling. Reconciliation jobs. Versioned data contracts. Strong identity controls.
That's also where one delivery partner can help if internal capacity is thin. For example, Cleffex Digital Ltd works on healthcare software integration and custom regulated platforms, which is relevant when a team needs support across architecture, interoperability, and delivery rather than isolated development tasks.
A Canadian enterprise platform doesn't become scalable because it's cloud-hosted. It becomes scalable when each new clinic, province, and partner can be added without redesigning the platform core.
Implementing a Practical AI and Data Strategy
Most healthtech AI plans are upside down. Teams start with use cases like summarisation, triage support, or forecasting, then discover their underlying data is fragmented, inconsistently labelled, or trapped in operational systems. That isn't an AI problem. It's a platform design problem.
In enterprise healthtech platform development, the data strategy needs to come first. AI sits on top of ingestion, storage, lineage, review, and monitoring. If those layers are weak, the model may still produce outputs, but the organisation won't trust or defend them.
Build the Data Path Before the Model Path
A practical stack starts with controlled ingestion from source systems such as EHRs, scheduling tools, portals, billing, and operational applications. From there, data should move into a governed storage layer where access, provenance, and transformation history are observable.
A sensible sequence looks like this:
Ingest With Provenance
Record where each dataset came from, under what connector, and with what timestamp or event context.Store in Governed Layers
Keep raw, normalised, and analytics-ready representations separate so teams can trace changes.Curate for Use Case Fit
Build feature-ready datasets for narrow operational or clinical workflows, not generic “AI-ready” warehouses.Serve Through Controlled Interfaces
Don't let models bypass platform security or pull data directly from unmanaged stores.
That structure matters because enterprise buyers increasingly want evidence, not ambition.
Governance Is Now Part of the Feature Set
Canada's proposed Artificial Intelligence and Data Act (AIDA) shifts the standard for high-impact AI. Buyers now look for operational readiness, not just model novelty. The practical controls include model audit trails, human-in-the-loop review, provenance tracking, and post-deployment monitoring, as described in this analysis of healthtech skills gaps and AI governance expectations.
That means AI architecture should answer questions like these:
What input data produced this recommendation?
Which model version generated it?
Was a human required to review before action?
Can the decision path be reconstructed later?
What happens when model behaviour drifts or source data changes?
If your team is designing those controls into the product, this guide to AI integration in healthtech platforms is a useful implementation reference.
Operational test: If a hospital asks you to explain how an AI output was produced and your answer depends on informal team knowledge, the system isn't enterprise-ready.
Pick Narrower Use Cases First
The first AI release should support a bounded workflow with a clear human owner. Good candidates are operational and administrative tasks where review can be structured, and the blast radius is limited. Bad candidates are broad, opaque features that cross multiple departments before the organisation has governance muscle.
I'd favour use cases that meet three conditions:
The inputs are already captured in structured or normalised form
A human already reviews the underlying workflow today
The platform can log decisions and exceptions cleanly
This keeps governance manageable and gives buyers confidence that the feature fits into existing accountability structures. In healthcare, trust comes from traceability and process discipline. Not from the model theatre.
Assembling Your Team and Managing the Project
The platform won't succeed because the architecture diagram is elegant. It succeeds because the right people make the right decisions at the right time. Healthtech projects go off track when one role is missing or when too many decisions sit with engineering alone.
For a first enterprise platform, you need a team that can balance product, clinical workflow, integration realities, and compliance constraints. That usually means fewer generalists than founders expect.
Core Roles You Actually Need
Some responsibilities can be combined in an early-stage team, but the functions themselves can't be skipped.
Product manager to prioritise workflows, manage trade-offs, and keep scope aligned with buyer value
Business analyst or workflow lead to document operational states, exceptions, and handoffs
Solution architect to own system boundaries, integration design, and security patterns
Backend and frontend engineers with experience in regulated applications and API-driven systems
QA lead who understands scenario-based testing, not just happy-path validation
DevOps or platform engineer to own environments, deployment discipline, secrets, and observability
Compliance or privacy leads to review controls, evidence requirements, and procurement responses
Clinical advisor or operational subject-matter expert to validate what happens in real settings
One of the most expensive mistakes is assuming the product manager or architect can “cover compliance later.” They can help, but regulated evidence work needs dedicated ownership.
Compare Sourcing Models Honestly
Different sourcing models fit different company stages. The right choice depends on how fast you need to move, how much domain expertise you already have, and whether this platform will become a long-term strategic asset inside the business.
| Factor | In-House Team | Fully Outsourced | Hybrid Model |
|---|---|---|---|
| Control over roadmap | Highest direct control | Lower day-to-day control | Shared control with internal ownership |
| Speed to assemble | Slower if hiring specialised roles | Faster if partner has ready capacity | Moderate |
| Access to niche expertise | Harder unless already hired | Strong if the vendor knows regulated delivery | Strong when gaps are targeted |
| Knowledge retention | Best long-term retention | Depends on documentation and handover | Better than full outsourcing |
| Cost flexibility | Less flexible in early stages | More flexible for fixed scopes or phases | Flexible if the scope is well managed |
| Best fit | Mature teams building a core long-term product | Companies needing fast execution and external depth | Teams that want strategic control with delivery support |
The Model I See Work Most Often
For a first Canadian enterprise platform, the hybrid model is usually the most resilient. Keep product ownership, workflow decisions, and key architecture control in-house. Bring in external specialists for integration, regulated engineering, DevOps maturity, or QA acceleration.
That structure prevents two common failures. First, internal teams don't get overwhelmed by specialist work, which they rarely do. Second, the company doesn't lose ownership of product knowledge and buyer context.
Project management should reflect healthcare reality. Don't run the programme as a generic sprint factory. Manage it around workflow milestones, integration dependencies, compliance evidence, and pilot readiness. A feature is not done because it passed QA. It's done when the workflow works with real users, real permissions, and real data conditions.
Your Go-to-Market Roadmap and Readiness Checklist
Canada's healthcare environment has been shaped by a federated model for years. Canada Health Infoway was launched in 2001 to accelerate digital health adoption across provincial and territorial systems, and that history matters because enterprise platforms in Canada must be designed around multi-jurisdiction integration from the start, not as a later enhancement, as noted in this overview of Canada's digital health platform context.
That changes the go-to-market plan. Your launch isn't just about shipping software. It's about proving the platform can operate across differing workflows, identity assumptions, and integration conditions without collapsing under customisation pressure.
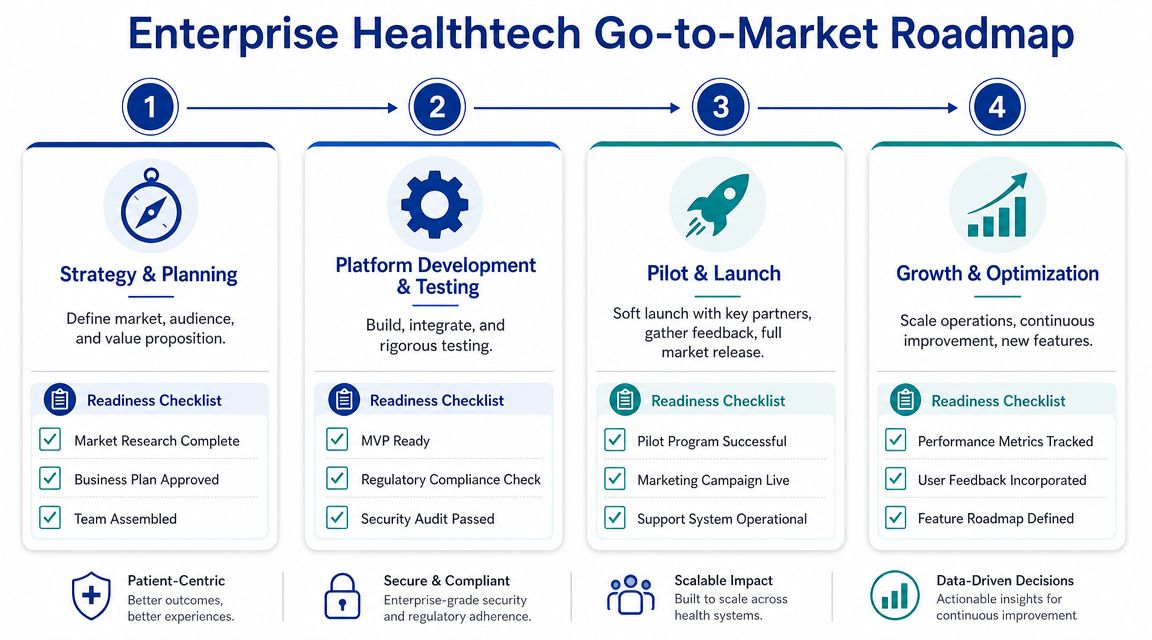
Phase the Rollout Around Risk, Not Ambition
A practical roadmap usually works best in four phases.
Strategy and Planning
Start with one target buyer profile and a narrow workflow spine. Define the initial jurisdiction assumptions, integration dependencies, security model, and procurement constraints before you scope the MVP.
Readiness questions:
Buyer clarity. Do you know whether the first customer is a clinic network, hospital group, insurer, or digital health operator?
Workflow focus. Have you chosen the smallest set of workflows that still proves enterprise value?
Jurisdiction fit. Have you identified which provincial realities affect launch requirements?
Platform Development and Testing
Build the platform core first. That means identity, permissions, auditability, canonical data handling, and core workflow orchestration. Leave broad feature expansion for later.
Use a hard gate before the pilot:
Controls implemented rather than documented only.
Primary integrations are working under expected edge cases.
Operational monitoring live for incidents, failures, and usage signals.
Launch readiness comes from proving the boring parts work under pressure. Authentication, logging, retries, data reconciliation, and support workflows decide whether pilots survive.
Pilot and Launch
Choose pilot partners carefully. The best pilot site is not the most prestigious organisation. It's the one willing to collaborate on workflow refinement, provide access to real operational stakeholders, and tolerate phased rollout discipline.
During the pilot, track qualitative signals such as:
whether staff can complete the workflow without local spreadsheets
whether support issues reveal training problems or design problems
whether integration exceptions are isolated or structural
Don't scale while core workflow ownership is still unclear.
Growth and Optimisation
Once the platform runs reliably in the first environment, expand by repeating a controlled integration and rollout pattern. Add adjacent capabilities such as portals, analytics, or AI only when the data and governance base is stable enough to support them.
A concise enterprise readiness checklist should cover all three layers:
| Area | Readiness check |
|---|---|
| Technical | canonical model defined, integration adapters tested, observability live, access controls enforced. |
| Regulatory | privacy controls implemented, audit evidence available, retention and disposal rules configured. |
| Operational | support ownership assigned, onboarding process documented, pilot feedback loop active, and change management in place. |
The strongest first launch is rarely the broadest. It's the one that solves a costly workflow problem, passes buyer scrutiny, and can be repeated in the next organisation without rebuilding the platform from scratch.
If you're planning an enterprise healthtech platform for the Canadian market, Cleffex Digital Ltd is one option to evaluate for regulated software delivery, healthcare integration, and AI-enabled platform development. The useful starting point is usually a scoped discovery around workflows, interoperability constraints, and compliance controls, so the build plan reflects operational reality rather than a generic product roadmap.







