



A patient arrives in your emergency department late on a Friday. The registrar has one record from the hospital EHR. The attending physician knows there's more history somewhere else. The patient saw a specialist across town, filled prescriptions at a retail pharmacy, and recently used a remote monitoring device at home. None of that is visible in one place.
So the team does what healthcare teams have done for years. They call, fax, log into separate portals, and make clinical decisions with partial information.
That's the setting where a healthcare data fabric starts to make sense. Not as another platform to buy, and not as a massive rip-and-replace programme, but as a practical way to connect what already exists. It gives clinicians, analysts, and operations teams a unified view of data that's still stored across many systems.
For large hospitals, that matters. For medium-sized provider groups, regional clinics, and health-tech startups, it may matter even more, because they usually can't afford a full rebuild of their infrastructure just to make data usable.
The Challenge of Disconnected Healthcare Data
The core problem isn't that healthcare lacks data. It's that healthcare has too much data in too many places, stored in too many formats.
A patient's journey might span an EHR, a lab system, PACS, billing software, a referral platform, a pharmacy feed, and wearable device data. Each system was often chosen for a good reason. But over time, the stack becomes fragmented. The result is familiar to every CIO. Clinical teams lose time, analysts wait on extracts, and IT spends its days stitching together interfaces.
What the fragmentation looks like in practice
In a medium-sized clinic network, one team may use one EHR module for encounters, another tool for imaging, and a separate application for scheduling and payments. The systems all work. They just don't work well together.
That disconnect creates three daily headaches:
Incomplete patient context: Clinicians see one version of the record, not the whole history.
Slow operational reporting: Finance, quality, and care management teams depend on manual data pulls.
Higher integration costs: Every new app needs another point-to-point connection.
A healthcare data fabric addresses this by acting like a universal translator for healthcare information. It doesn't require every source system to be replaced. It creates a layer across them, so users can access and understand data through a unified structure.
A good fabric doesn't force every system to speak the same native language. It translates meaning at the point of use.
That distinction matters. Many leaders still assume integration means migration. In a fabric architecture, much of the value comes from connecting, standardising, and governing data without moving everything into one giant repository first.
Why it has become a board-level issue
This isn't a niche architecture discussion any more. The healthcare data fabric market was valued at $2.1 billion in 2022 and is projected to reach approximately $8.9 billion by 2032, with a CAGR of 15.54% from 2023 to 2032. North America is projected to hold a 30.00% share in 2025, according to this healthcare data fabric market analysis.
That growth reflects a shift in priorities. Healthcare organisations aren't just trying to store data. They're trying to activate it for care coordination, analytics, and AI.
If you're already evaluating interoperability strategy, broader connected healthcare platforms often sit beside data fabric discussions because both aim to make fragmented care delivery more usable and more coordinated.
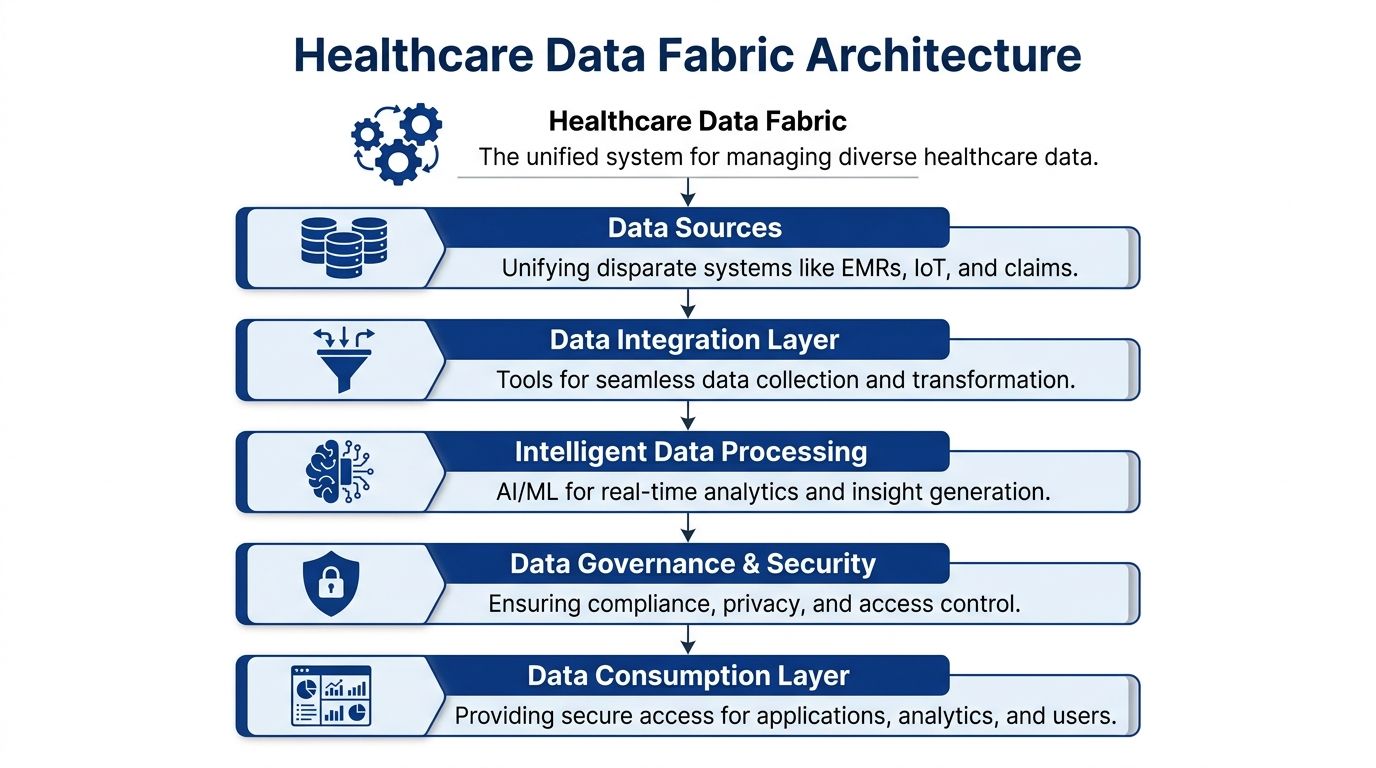
Core Architecture and Key Components
A healthcare data fabric isn't one product box with a single logo on it. It's an architectural approach. Think of it as a digital nervous system that senses where data lives, understands what it means, and makes it available securely to the right people and applications.
This is the visual model often needed before the term starts to feel concrete.
Data virtualisation
The first idea to grasp is access without forced relocation.
In many environments, data stays where it already lives. The fabric uses APIs, connectors, and query services to reach into source systems and present data through a common access layer. That means your Epic environment, imaging archive, claims database, or device feed doesn't always need to be copied into a new home before it becomes useful.
For a CIO, this is often the first relief point. You don't need a multi-year migration just to start solving interoperability problems.
Semantic layer and knowledge graph
Raw data fields aren't enough. Healthcare needs context.
A semantic layer maps different source terms and structures to a common meaning. For example, one system may store diagnosis information one way, another may organise encounters differently, and a third may label medication fields inconsistently. The semantic layer helps the fabric recognise that those records may describe the same patient, event, or concept.
A knowledge graph adds relationship awareness. It helps the architecture understand links among patients, providers, episodes, orders, devices, and outcomes.
Practical rule: If your architecture can retrieve data but can't explain what the data means, you haven't solved interoperability. You've just sped up confusion.
Catalogue, metadata, and policy automation
Once data is connected, people still need to find it.
That's the role of the data catalogue. It gives analysts, application teams, and governance staff a searchable inventory of available datasets, definitions, lineage, and ownership. Instead of asking IT where a trusted discharge dataset lives, a user can locate the governed source directly.
Metadata then becomes more than documentation. It becomes operational.
Active metadata tracks lineage: Teams can see where data came from and how it changed.
Policy metadata enforces rules: Access, masking, and retention policies can be applied consistently.
Operational metadata improves reliability: Platform teams can spot failures, stale pipelines, or schema drift faster.
For organisations comparing design options, these patterns align with broader enterprise application architecture patterns because the fabric usually sits across existing applications rather than replacing them outright.
Open standards matter more than vendor branding
In healthcare, architecture quality often depends less on the dashboard and more on the standards underneath. Open standards such as HL7 FHIR and DICOM are what make a fabric durable. They let you connect current systems and future tools without locking every workflow into one vendor stack.
That's why the strongest fabric designs are usually the least theatrical. They focus on connectors, semantics, metadata, APIs, identity controls, and standards. Quiet infrastructure. Big downstream effect.
Unlocking Tangible Benefits for Healthcare Providers
The architectural story matters, but a CIO still has to ask a harder question. What changes on Monday morning after a healthcare data fabric goes live?
The answer is usually operational before it becomes visionary. Reporting gets faster. Analysts spend less time reconciling mismatched extracts. Clinical and administrative teams stop chasing the same data across separate systems.
According to this overview of healthcare data fabric outcomes, a healthcare data fabric can reduce clinical reporting latency by 40 to 60 per cent, cut manual data reconciliation effort by over 70 per cent, and reduce data discovery time from weeks to minutes.
Where the value shows up first
The first wins are often unglamorous, which is exactly why they matter.
A quality reporting team that used to wait for data from multiple source systems can move faster because the fabric exposes governed, API-driven access to the same information. A care management team can work from a more complete view of encounters and follow-up activity. A data science team can spend less time cleaning source variation and more time testing models.
Those changes tend to affect four groups right away:
Clinical operations teams: They get timelier reporting and fewer blind spots.
Revenue and finance leaders: They spend less effort reconciling data from billing, claims, and encounter systems.
Analytics teams: They can discover and trust data faster.
AI programme owners: They can work from more standardised pipelines instead of one-off extracts.
Why medium-sized organisations benefit differently
Large health systems often justify data fabric investments as enterprise transformation. Mid-market provider groups and startups usually need a tighter business case.
For them, the value often comes from avoiding complexity. They don't want five new platforms. They want one architecture that helps existing systems cooperate. If their clinic can connect note data, imaging metadata, and scheduling records without a complete rebuild, that's progress. If governance improves at the same time, even better.
A useful way to think about ROI is this:
| Operational problem | Typical pre-fabric reality | Post-fabric improvement |
|---|---|---|
| Reporting delays | Teams wait on extracts and manual joins | Reports move faster through unified access |
| Data reconciliation | Staff compare multiple sources by hand | Standardised access reduces manual effort |
| Data discovery | Analysts search across teams and folders | Catalogue and metadata make trusted data easier to find |
| AI readiness | Projects stall on inconsistent inputs | Standardised pipelines support model development |
The real gain isn't just speed. It's fewer decisions made from incomplete or conflicting data.
That's why a healthcare data fabric should be treated as core operating infrastructure. Not as a side innovation project, and not as a dashboard initiative wearing a bigger name.
Real-World Healthcare Data Fabric Use Cases
Use cases are where the term stops sounding abstract. A healthcare data fabric becomes easier to evaluate when you can see where it fits in daily care delivery, research, and operations.

Population health and care coordination
A regional provider group wants to identify patients with gaps in follow-up care after discharge. The necessary information sits across admission records, discharge summaries, scheduling tools, and sometimes external referral systems.
Without a fabric, the team often builds a fragile reporting process around extracts. With a fabric, they can query a unified view of those events and relationships. The care management team gets a cleaner list of patients who need outreach, and the quality team works from the same underlying definitions.
This kind of use case matters because it depends on relationships, not just records. You need to connect people, events, timing, and responsibility across systems that weren't designed together.
Clinical research and cohort discovery
Research teams face a different version of the same problem. They may need to identify patients who meet very specific criteria across diagnoses, treatments, imaging history, and laboratory results.
A healthcare data fabric helps because it exposes governed access to distributed data while preserving meaning. Researchers don't need to hunt for separate exports from every department before they can even test feasibility. The architecture makes cohort identification more practical and more repeatable.
For teams building retrieval pipelines on top of fragmented medical content, tools such as Web Scraping API for RAG can also be useful when external medical or operational content needs to be collected and normalised for AI workflows alongside internal datasets.
AI note enrichment for smaller clinics
This is the use case many enterprise articles miss.
A medium-sized clinic or startup may not need a giant enterprise lakehouse first. It may wish to enrich unstructured physician notes, intake forms, and imaging metadata so records become more searchable and useful.
That's where a healthcare data fabric can be a practical enabler. According to this analysis on AI and healthcare data silos, 50 to 90 per cent of healthcare data is siloed and unstructured, and a fabric can make that data accessible for smaller clinics using open standards such as FHIR and DICOM without massive proprietary infrastructure spending.
A realistic scenario looks like this:
Source data: Free-text notes, scanned documents, image metadata, and device observations.
Fabric role: Connect, standardise, tag, and govern those inputs.
AI layer: Extract symptoms, medication changes, follow-up needs, or imaging references.
Business outcome: Better search, cleaner records, and more usable context for clinicians.
Smaller organisations usually don't need more infrastructure first. They need cleaner paths between the tools they already have.
That's the underappreciated strength of the model. A healthcare data fabric can support ambitious use cases without demanding a complete technical reset.
Navigating Compliance, Security, and Integration
Security teams often hear “more connected data” and assume “more risk”. In a poorly designed environment, that concern is justified. In a well-designed healthcare data fabric, the opposite can be true.
The reason is simple. Fragmented systems often produce fragmented governance. Each application has its own access rules, audit approach, and integration logic. That makes compliance harder to prove and harder to manage.

Why centralised governance helps
A healthcare data fabric can create one policy-aware layer across many systems. That allows security and compliance teams to define access controls, lineage rules, and audit requirements more consistently.
According to this healthcare payer fabric compliance discussion, deploying a data fabric aligned with HIPAA and HITRUST can reduce infrastructure duplication costs by 35 per cent, ensure 100 per cent audit trail completeness for all data access events, and cut data quality anomaly rates by 52 per cent.
Those are meaningful outcomes because they address three common failure points at once:
Too many duplicate data environments
Audit gaps across disconnected tools
Data quality issues that spread downstream
Compliance isn't separate from architecture
Healthcare leaders sometimes treat compliance as a review gate after design work is done. That usually leads to rework.
A better approach is to build compliance into the architecture itself. Role-based access control, minimum necessary access, lineage capture, retention policies, and consent-aware integration patterns need to be part of the fabric design from the start.
If your security team is formalising validation processes around PHI handling, this guide to penetration testing for HIPAA compliance is a useful companion because it addresses the testing discipline that should sit beside architectural controls.
Integration without locking yourself in
The integration side matters just as much as the governance side. A fabric that only works cleanly with one cloud stack or one proprietary data model can become tomorrow's bottleneck.
Open standards reduce that risk. HL7 FHIR supports cleaner exchange for clinical data. DICOM matters for imaging workflows. API-driven access keeps downstream applications from depending on brittle batch extracts alone.
A sound pattern usually includes:
Existing EHR and operational systems as systems of record
A semantic and integration layer for standardised access
Central policy enforcement for identity, masking, and auditability
Reusable APIs and governed datasets for apps, analytics, and AI
For leaders reviewing broader risks around protected data, this overview of data security in healthcare information systems gives useful context on how security architecture and operational controls need to work together.
If auditors ask who accessed which data, when, and under what policy, your fabric should answer that directly, not through detective work across five platforms.
That's when interoperability and compliance stop fighting each other. They start reinforcing each other.
Your Implementation Roadmap and Vendor Selection
Most healthcare organisations fail with new data architecture for a boring reason. They start too wide.
A healthcare data fabric works best when it begins with a focused operational problem, proves value, and expands through governed reuse. The target isn't a perfect future state diagram. The target is a working capability that solves a real bottleneck.
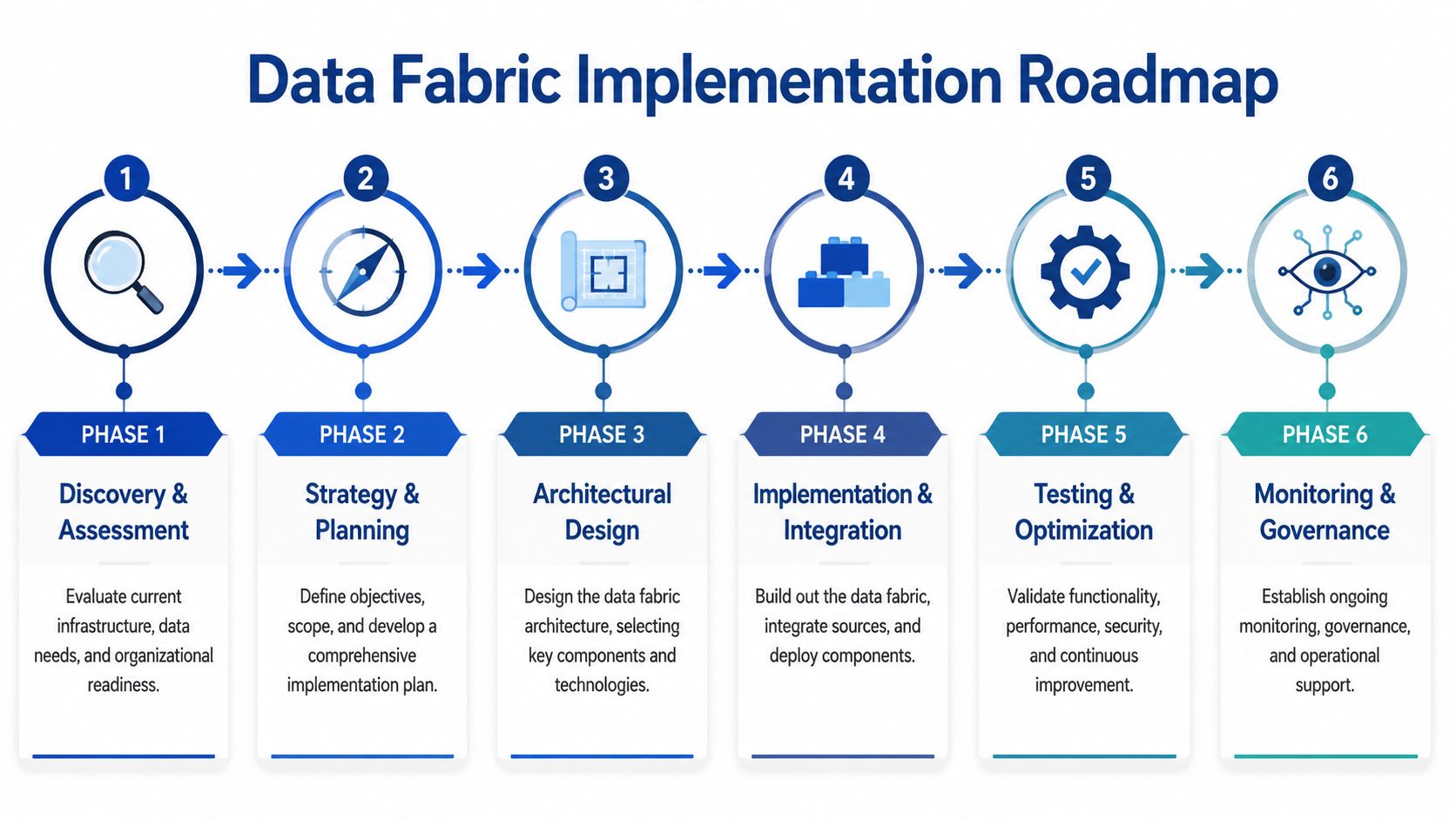
A phased roadmap that stays manageable
A practical rollout usually looks like this:
Discovery and assessment
Inventory your critical data sources, interfaces, reporting pain points, and compliance obligations. Don't catalogue everything equally. Prioritise data tied to care coordination, reporting delays, and AI use cases.Strategy and scope
Choose one use case that matters to both business and technical teams. Good candidates include discharge reporting, provider quality reporting, or note enrichment in a clinic network.Architecture design
Define how virtualised access, semantic mapping, identity controls, and metadata management will work in your environment. Decide early where open standards such as FHIR and DICOM will be the default integration path.Pilot implementation
Build only what the pilot needs. Connect a small number of systems. Validate access controls, lineage, and data quality before expanding to broader use.Operational hardening
Test reliability, permissions, monitoring, and support workflows. A pilot that works only when two architects are watching it isn't ready.Scale and governance
Add more domains once teams trust the first one. Growth should follow reusable patterns, not one-off exceptions.
Questions to ask before selecting a vendor
Vendor selection often goes wrong when buyers focus on feature lists instead of architectural fit. In healthcare, the right partner needs to understand standards, compliance realities, and incremental delivery.
Here's a practical scorecard.
| Criterion | Description | Why It Matters |
|---|---|---|
| Interoperability support | Ability to work with FHIR, DICOM, APIs, legacy interfaces, and hybrid environments | Healthcare data is spread across modern and legacy systems |
| Virtualisation capability | Access to data without forcing immediate migration | Reduces disruption and speeds early wins |
| Semantic modelling | Support for common definitions, mappings, and relationship-aware data models | Turns disconnected fields into usable clinical and operational context |
| Metadata and lineage | Strong catalogue, discovery, lineage, and policy automation features | Makes governance and auditability workable at scale |
| Security controls | Role-based access, masking, auditing, and policy enforcement | Required for PHI protection and operational trust |
| Deployment flexibility | Fit for cloud, on-premises, or mixed environments | Many organisations can't standardise on one hosting model |
| Healthcare expertise | Proven understanding of provider, payer, clinical, and compliance workflows | Reduces translation errors between technology and operations |
| Implementation approach | Willingness to start with a pilot and expand iteratively | Lowers risk and avoids over-engineering |
| Support model | Clear ownership for deployment, training, maintenance, and optimisation | Fabric programmes fail when handoff is vague |
A final buying filter
Ask every vendor one blunt question: How do you help us connect existing systems without forcing a wholesale rebuild?
If the answer is mostly about migration, pause. If the answer includes standards, virtualisation, metadata, phased delivery, and governance, you're probably in a better conversation.
Measuring Success and the Future of Connected Care
A healthcare data fabric should be measured by what it changes, not by how elegant the architecture diagram looks.
Start with a small KPI set that operations, clinical leadership, and IT all recognise as meaningful:
Time to data access for analysts and reporting teams
Manual reporting effort across quality, finance, and operations
Data quality improvement based on fewer anomalies and cleaner lineage
Access governance performance such as audit readiness and policy consistency
AI readiness based on whether teams can obtain trusted, standardised inputs without custom extraction work
Those measures matter because connected care depends on them. If teams still can't find trusted data, still spend hours reconciling reports, and still build one-off pipelines for every model, the architecture hasn't solved the core problem.
The future angle is straightforward. Safe healthcare AI needs timely, contextual, governed data. Generative AI, summarisation tools, operational copilots, and decision support systems all depend on a layer that can connect and standardise fragmented information without weakening compliance.
That's why the healthcare data fabric is becoming foundational. It isn't just an integration tactic. It's the operating model for organisations that want more coordinated care, stronger governance, and practical AI adoption without tearing out everything they already run.
If your organisation is planning a healthcare data fabric initiative, modernisation project, or secure AI rollout, Cleffex Digital Ltd can help you design and deliver pragmatic solutions that fit existing systems, compliance requirements, and growth goals. Their teams work with clinics, hospitals, startups, and mid-market enterprises that need interoperable software, cloud architecture, and AI-ready platforms without unnecessary complexity.







