



The leadership team usually starts talking about operations after a painful quarter.
Claims are delayed. Nurses are covering gaps with overtime. Managers are stitching together reports from the EHR, the billing system, spreadsheets, and email threads. Patients don't see that internal chaos directly, but they feel it in long waits, missed follow-ups, and hand-offs that don't quite land. That's the moment many organisations realise they don't have a staffing problem alone, or a scheduling problem alone, or a reporting problem alone. They have an operating model problem.
That's where HealthcareOps solutions become useful. Not as another platform to buy and bolt on, but as a way to redesign how work flows across clinical, administrative, and patient-facing teams. The best investments improve cost control, reduce friction, and make care delivery more reliable without asking staff to become system integrators in their spare time.
Why HealthcareOps Solutions Are No Longer Optional
Most hospitals and multi-site care groups are running into the same wall. Revenue cycle teams want cleaner workflows. Clinical leaders want fewer clicks and fewer workarounds. Operations wants visibility. Finance wants a credible cost case. Everyone wants those outcomes at once, but the underlying systems were often purchased at different times, for different departments, with different assumptions.
That patchwork used to be tolerable. It isn't now. In the US market, medical costs rose an average of 7% annually from 2021 to 2024, and pharmacy costs rose 9% annually over the same period, according to McKinsey's outlook for US healthcare. When costs keep climbing at that pace, manual administration stops being an inconvenience and becomes a strategic risk.
The Pressure Is Operational, Not Just Financial
Rising costs don't hit one line item. They hit the whole operating chain.
Front office teams end up re-entering data because systems don't share context cleanly.
Care managers chase status updates across inboxes and disconnected dashboards.
Department leaders spend too much time reconciling reports instead of fixing bottlenecks.
Clinicians absorb the failure points when scheduling, authorisation, and follow-up processes break.
A lot of leadership teams respond by shopping for a single tool. That's understandable, but it often creates another silo. A staffing team may start with the best hospital scheduling app because shift coverage is visibly painful, and that can be a sensible first move. The mistake is treating that purchase as the whole strategy instead of one layer in a broader operating model.
Why Timing Matters Now
Healthcare organisations heading into a major operational technology investment need to think in terms of system design. That means process ownership, data quality, integration rules, adoption planning, and governance. Software matters, but operating discipline matters more.
Practical rule: If your team can't explain how a workflow moves across departments today, technology won't fix it tomorrow.
A useful starting point is to align the work with a broader digital transformation approach in healthcare so the investment supports long-term operating change rather than a short-term patch. The organisations that move first usually aren't chasing novelty. They're trying to stop expensive friction from becoming normal.
Demystifying HealthcareOps: A Unified Framework
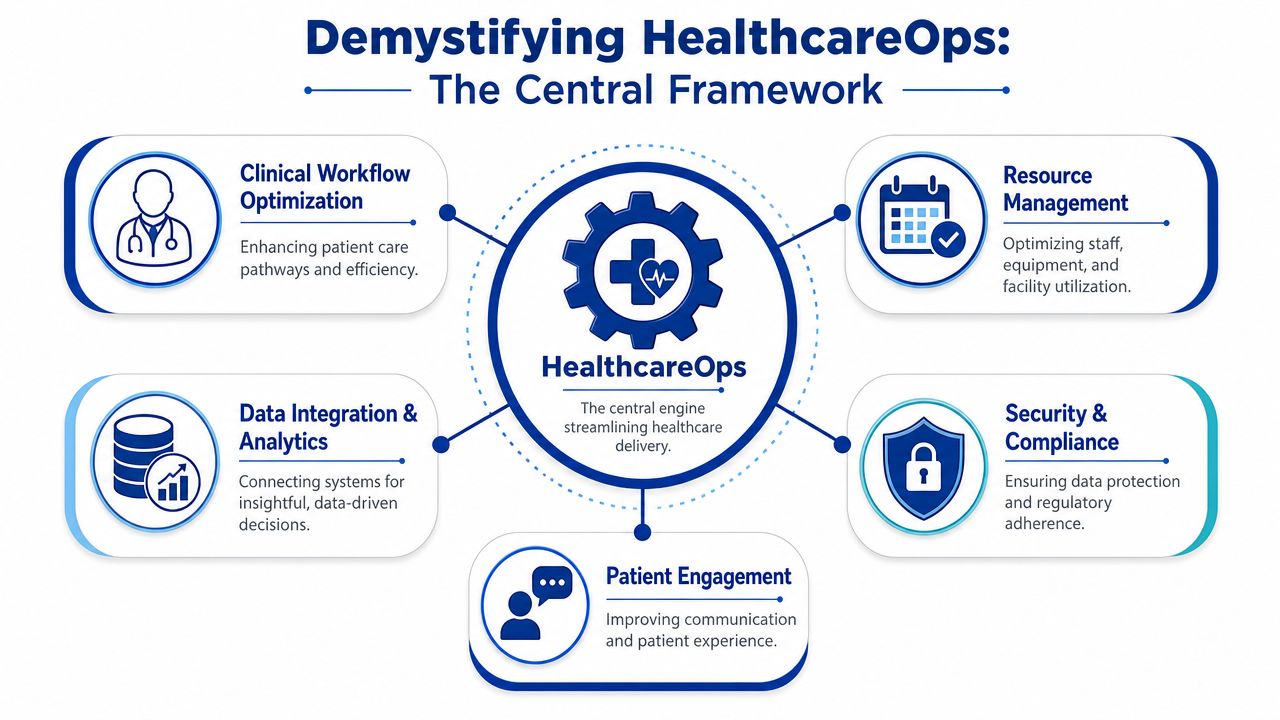
HealthcareOps is easiest to understand as a digital nervous system for the organisation. It senses what is happening across the enterprise, routes information to the right place, and helps people act without waiting for another manual hand-off.
That matters because most care organisations don't fail from lack of effort. They fail due to poor coordination. The billing team sees one version of the patient journey, the clinic sees another, and the patient experiences the gaps between them. HealthcareOps solutions aim to close those gaps by unifying process, data, and accountability.
Here's the framework in one view.
Think in Pillars, Not Products
A mature HealthcareOps model usually brings together five practical pillars:
Clinical workflow optimisation so staff can move through intake, treatment, discharge, and follow-up with fewer manual jumps.
Resource management covering people, rooms, devices, and time slots.
Data integration and analytics to create a shared operating picture.
Security and compliance ensure that access, auditability, and controls aren't left to chance.
Patient engagement to make communication, reminders, and navigation part of operations, not an afterthought.
This is why buying a point solution rarely solves the whole problem. You may improve one workflow while making another harder to manage.
Why the Category Has Grown So Quickly
The market signal is strong. The population health management solutions market, which sits close to the core of HealthcareOps, was valued at USD 28.5 billion in 2022 and is projected to reach USD 115.6 billion by 2032, according to Global Market Insights. That doesn't mean every product is good. It does mean healthcare organisations are investing heavily in coordinated operations, data use, and implementation support.
One practical lesson from that growth is this. Leaders shouldn't ask, “Which software do we buy?” first. They should ask, “Which operating capabilities do we need to make dependable?”
For patient access and service workflows, teams can also learn from adjacent operational models, such as a platform for efficient contact centres, because contact routing, queue design, and unified communication are often central to access performance in healthcare as well.
HealthcareOps works best when leaders treat it as an enterprise discipline. Not a department tool.
If your team is still framing the initiative as an IT deployment, it helps to review how connected healthcare platforms support shared workflows across care, operations, and patient communication. Its value comes from coordination.
The Core Components of a Modern HealthcareOps Platform
A modern HealthcareOps platform is less about flashy features and more about whether the foundation can support real operational load. If I'm advising a hospital on first investment priorities, I look for five components. Not because they sound complete in a vendor slide, but because missing any one of them usually creates expensive rework later.

Interoperability That Is Actually Testable
Every vendor says they integrate. That statement means very little until you ask how.
True interoperability depends on standards-based architecture. The HL7-OMG Healthcare Services Specification Project formalised service models and technical specifications that were adopted as standards in 2008, making integration across clinical systems more testable and less ambiguous, as described in the HL7-OMG HSSP overview.
When interfaces are improvised, each upgrade becomes a negotiation. When interfaces are standardised, each upgrade becomes manageable.
What matters in practice is whether the platform can support clean service definitions, conformance, and predictable data exchange across EHR, billing, scheduling, and care coordination systems.
Security and Compliance Built Into Workflow
Security isn't a separate workstream with healthcareops solutions. It sits inside identity, permissions, audit logs, messaging, and data movement. If the platform only addresses compliance after process design, staff will invent workarounds, and those workarounds usually become the actual system.
Look for architecture that supports role-based access, clear auditability, and data segregation where needed. The question isn't only whether the system is secure. It's whether secure behaviour is the easiest behaviour for staff.
Automation That Removes Low-Value Work
Good automation takes repetitive administrative steps away from teams without hiding critical exceptions. Examples include routing prior authorisation tasks, matching referrals to the correct queue, triggering follow-up communication, and surfacing missing documentation before a claim stalls.
Bad automation does the opposite. It masks broken processes and pushes unresolved edge cases back to staff in more confusing ways.
Analytics Tied to Operating Decisions
Reporting alone isn't enough. Leaders need analytics that tell them what action to take. A dashboard is useful only when it helps answer questions such as where bottlenecks form, which locations are drifting from standard practice, or which workflows create unnecessary delay.
The strongest platforms link analytics to ownership. Someone should know who responds when a threshold slips.
Virtual Care and Distributed Access Support
Telehealth enablement belongs inside the operational stack when it affects scheduling, follow-up, messaging, and documentation. It shouldn't sit on the edge as a standalone digital front door with no operational backbone behind it.
A useful evaluation lens is whether the platform supports a coherent care operations model across in-person and remote interactions. If it doesn't, patients will feel the break, even if the video visit itself works fine.
For a broader architectural lens, this guide to the modern CareOps tech stack is a helpful companion when defining what belongs in the core platform versus what should remain modular.
Your Implementation Roadmap From Strategy To Launch
Most failed HealthcareOps programmes don't fail at launch. They fail earlier, during framing. The organisation buys technology before it decides which operating decisions the technology must support. That creates a familiar pattern. Scope expands, timelines slip, adoption stalls, and the project gets judged as a software problem when it was really a strategy problem.
The better route is cyclical. Build the foundation, launch in phases, and keep refining.
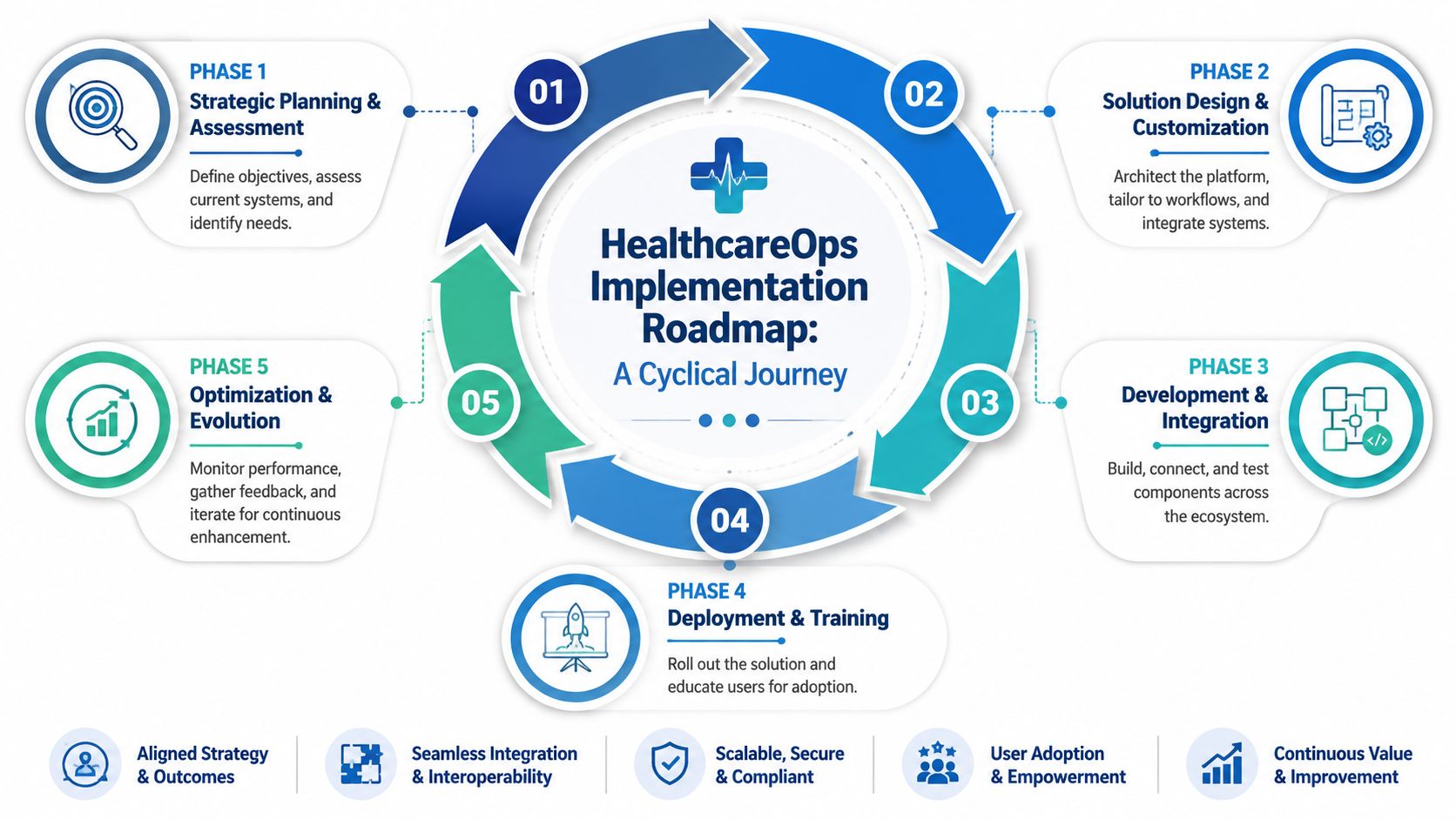
Start With the Business Case, Not the Feature List
A sound business case answers four questions.
Which operational failures cost us the most?
Delayed throughput, poor hand-offs, excess manual work, avoidable denials, or fragmented patient communication.Which workflows cross departmental boundaries?
Those are usually the ones worth fixing first, because that's where hidden friction lives.Which measures will prove progress?
Pick a small set that finance, operations, and clinical leadership all accept.Which constraints are essential?
Security, compliance, integration rules, and change capacity need to be explicit.
This early work is where many teams discover they've been discussing symptoms, not root causes.
Design the Foundation Before Adding Intelligence
Deloitte's 2025 outlook argues that successful digital transformation depends on a linked stack of modern data infrastructure, cloud migration, and cybersecurity hardening before organisations layer on advanced AI or workflow automation, as noted in Deloitte's 2025 health care outlook.
That sequencing is practical. If your data is inconsistent, your integration model is brittle, or your security controls are immature, adding AI accelerates confusion.
Decision test: If a process owner can't trust the source data, don't automate that process yet.
Roll Out by Operational Domain
Don't launch enterprise-wide if your organisation hasn't yet proved adoption in one high-friction domain. Phased rollout works better when each phase has a clear owner and a bounded workflow.
Examples include:
Access and scheduling first when no-show management, queue control, and intake delays are hurting throughput.
Revenue cycle first; when denials, missing documentation, or hand-off failures are affecting cash flow.
Care coordination first when discharge, referral, or follow-up workflows are fragmented.
Each phase should include workflow redesign, not just system configuration.
Treat Adoption as Part of the Build
Training delivered at the end rarely sticks. Users need role-specific guidance, local champions, and visible feedback loops. Managers also need to know what to stop doing manually once the new workflow is live. Otherwise, the organisation ends up running old and new processes in parallel.
One practical option is to work with partners that can handle custom software, integration, and workflow design together. For example, Cleffex Digital Ltd develops healthcare-focused software and enterprise custom solutions, which can fit organisations that need customised operational workflows rather than an off-the-shelf package alone.
Keep Optimisation Funded
A launch isn't the finish line. Once the platform is live, review where workarounds reappear, where data quality drops, and where teams still rely on side spreadsheets. Those signals tell you what the operating model still hasn't absorbed.
Choosing the Right HealthcareOps Partner
Leadership teams often compare vendors on demos. That's not enough. A polished demo can hide weak implementation discipline, shallow healthcare knowledge, or a support model that disappears once the contract is signed.
A better evaluation method is to push potential partners into operational specifics. Ask them how they handle workflow redesign, integration ownership, security decisions, role-based adoption, and post-launch accountability. If the answers stay generic, that's useful information.
Questions That Separate Real Partners From Software Resellers
| Criterion | Why It Matters | Red Flags to Watch For |
|---|---|---|
| Healthcare domain understanding | Healthcare workflows have clinical, administrative, and compliance dependencies that generic enterprise software teams often miss. | They talk mainly about product features and struggle to map those features to referrals, discharge, scheduling, claims, or care coordination. |
| Integration capability | Most value depends on connecting EHR, billing, scheduling, communication, and reporting tools without fragile workarounds. | They promise “easy integration” but can't explain ownership, testing, failure handling, or standards approach. |
| Security and compliance discipline | Access control, auditability, and data handling decisions shape day-to-day operational risk. | Security is described as a separate module rather than part of the workflow and architecture design. |
| Change management model | Staff adoption determines whether the platform becomes the real operating system or an extra layer everyone avoids. | Training is limited to go-live sessions, with little mention of super users, feedback loops, or role-specific support. |
| Post-implementation support | Healthcare operations change continuously. Your partner should support optimisation, not just deployment. | Their support model ends at launch or depends on expensive change requests for routine operational improvements. |
| Scalability of architecture | Today's use case may be staffing or access, but tomorrow's may include analytics, remote care, or new locations. | The design works for a pilot but looks rigid when multi-site governance, new workflows, or added systems come into scope. |
What To Ask in the Room
Use direct questions.
“Show us how you'd model one of our cross-department workflows.”
“Who owns integration testing when systems change?”
“What governance do you expect from us internally?”
“How do you handle adoption when one department moves faster than another?”
“What happens after launch in months two through six?”
A good partner won't promise a frictionless implementation. They'll show you where the friction will be and how they plan to manage it.
That honesty matters more than a broad feature set. In HealthcareOps, the costliest mistake is choosing a partner that can sell software but can't help you change how work gets done.
Measuring Success and Common Pitfalls To Avoid
Many teams measure HealthcareOps success too narrowly. They focus on efficiency alone. Time saved matters, but it's not the whole return. A hospital can reduce clicks and still leave patients struggling to access care. It can automate routing and still burn out staff if governance is weak and exceptions pile up.
A better scorecard includes efficiency, clinical operations, workforce experience, and patient access.

What To Measure After Go-Live
Start with metrics that reveal whether work is flowing more cleanly.
Operational flow: Are hand-offs faster, queues clearer, and exception paths easier to manage?
Financial discipline: Are leaders getting cleaner operational visibility that helps them act sooner?
Staff experience: Are managers and frontline users relying less on duplicate work and manual chasing?
Patient access and continuity: Are outreach, follow-up, and navigation improving for patients who usually fall through gaps?
The last point is often missed. Social determinants such as food, housing, transportation, and education account for about 40% of what drives poor health, according to the AAMC discussion of underserved populations. If your implementation only improves internal workflow while ignoring access barriers, the operational model is incomplete.
Common Mistakes That Get Expensive Fast
The most common failure modes are predictable.
Poor data hygiene: Teams automate around inconsistent names, codes, statuses, and ownership rules. The platform then scales confusion faster.
No process redesign: Leaders digitise a broken workflow and call it a transformation.
Weak clinician and manager buy-in: Adoption drops when teams feel the system was imposed rather than designed around real work.
Overbuilt first release: Too much scope creates testing problems, training problems, and accountability problems.
Equity blind spots: Organisations improve dashboards without improving how underserved patients move through access points.
A More Realistic View of ROI
ROI in HealthcareOps isn't only about reducing administrative effort. It's also about creating a more dependable operating environment. When teams know where work sits, who owns the next step, and where exceptions go, they make better decisions with less friction.
That's also why workforce thinking belongs in the conversation. Software can remove low-value work, but it can't replace local talent development. In Los Angeles, Children's Hospital Los Angeles says its CHAMP programme has enabled nearly 300 students to gain exposure to healthcare careers since 2013, according to Children's Hospitals Today. Operational resilience often comes from combining workflow technology with stronger staffing pipelines, especially in communities where access is already fragile.
Don't ask only whether the system made work faster. Ask whether it made care delivery more reliable for the people most likely to be missed.
The Future of Healthcare Is Operational Excellence
HealthcareOps isn't a passing category label. It reflects a deeper shift in how healthcare organisations have to run. Cost pressure, fragmented systems, workforce strain, and patient access challenges all point to the same conclusion. Operational excellence is now a strategic capability.
The organisations that get this right won't be the ones with the most software. They'll be the ones who build a coherent operating model. They'll sequence the investment properly, choose partners carefully, and measure success in ways that reflect both internal performance and patient reality.
That work usually starts with a simple move. Assess where your biggest operational friction lives, then design from there. HealthcareOps solutions are most valuable when they connect business discipline with clinical reality.
If your team is evaluating a first major HealthcareOps investment, Cleffex Digital Ltd can be a practical partner to explore. Cleffex builds custom software, cloud, AI, and healthcare-focused digital solutions that can support workflow redesign, integration planning, and secure operational platforms for hospitals, clinics, and healthcare businesses.







