



A patient with a chronic condition rarely sees a single provider. They might see a family doctor, a specialist, a physiotherapist, and a pharmacist, while also using a blood pressure monitor or glucose device at home. The problem isn't a lack of data. It's that the data often sits in separate systems, arrives late, or never reaches the person who needs it.
Hospital administrators and clinic owners feel this fragmentation every day. Staff re-enters data. Clinicians switch between portals. Patients repeat their history. A remote reading may exist, but if it doesn't reach the EMR, the care team can't act on it with confidence. That's where connected healthcare platforms matter. They don't just add another app. They create a usable operational layer across appointments, clinical records, devices, messaging, and patient-facing services.
For Canadian buyers, this has shifted from a digital ambition to an infrastructure decision. The organisations getting value from connected care aren't the ones buying the flashiest dashboard. They're the ones building a reliable flow of information across systems, teams, and care settings.
The Future of Integrated Patient Care Is Here
A familiar scenario plays out in many Canadian care settings. A patient checks blood pressure at home. Their specialist wants trend data. Their family doctor wants medication adherence notes. The clinic receptionist is trying to confirm a virtual follow-up, while the patient is also using a portal to request a refill. Each piece exists, but the workflow still feels disconnected.
That gap is exactly what connected healthcare platforms are built to close. They unify patient information, communication, and action points so care teams don't have to chase data across separate products. In practice, that usually means bringing together online appointments, e-prescriptions, patient portals, remote monitoring feeds, and clinical system integrations into one coordinated environment.
Canada has moved decisively in this direction. During the COVID-19 era, connected healthcare platforms gained momentum as health systems expanded virtual care, and a key milestone was the federal investment of CAD 200 million in 2020 for Canada Health Infoway to accelerate digital adoption across provinces and territories, helping normalise online appointments, e-prescriptions, and patient portals according to this Canadian digital health review.
What Buyers Are Really Looking For
Most administrators aren't asking for “digital transformation” in the abstract. They're asking practical questions:
Can clinicians see the right patient data quickly enough to act on it?
Will this reduce admin friction or create more of it?
Can the platform work with our existing EMR and device mix?
Will patients use it without support calls rising every week?
Those are the right questions.
A connected platform works when it supports care continuity. It fails when it becomes a thin visual layer on top of disconnected systems. Buyers should treat it as part clinical workflow engine, part integration strategy, and part patient access layer.
A connected healthcare platform only matters if it improves decisions and reduces hand-offs. If staff still have to copy, chase, and reconcile data manually, the platform hasn't solved the real problem.
The operational foundation matters as much as the software itself. For organisations reviewing infrastructure and service partners, broader support around networks, devices, endpoint reliability, and uptime also affects platform success. That's why healthcare teams often pair platform planning with a review of managed IT for healthcare services, especially when multiple sites or device fleets are involved.
For organisations exploring a connected care strategy, it helps to start with a partner that understands software, integration, and delivery realities in Canada.
Deconstructing Connected Healthcare Architecture
If you strip away the marketing language, a connected healthcare platform is a central nervous system for healthcare operations. It gathers signals from many sources, routes them securely, interprets them, and presents the right information to the right person.
The architecture matters because weak foundations create expensive problems later. A platform may look polished in a demo, but if it can't ingest device data cleanly, synchronise patient identity, and expose interoperable interfaces, it won't hold up under day-to-day clinical use.
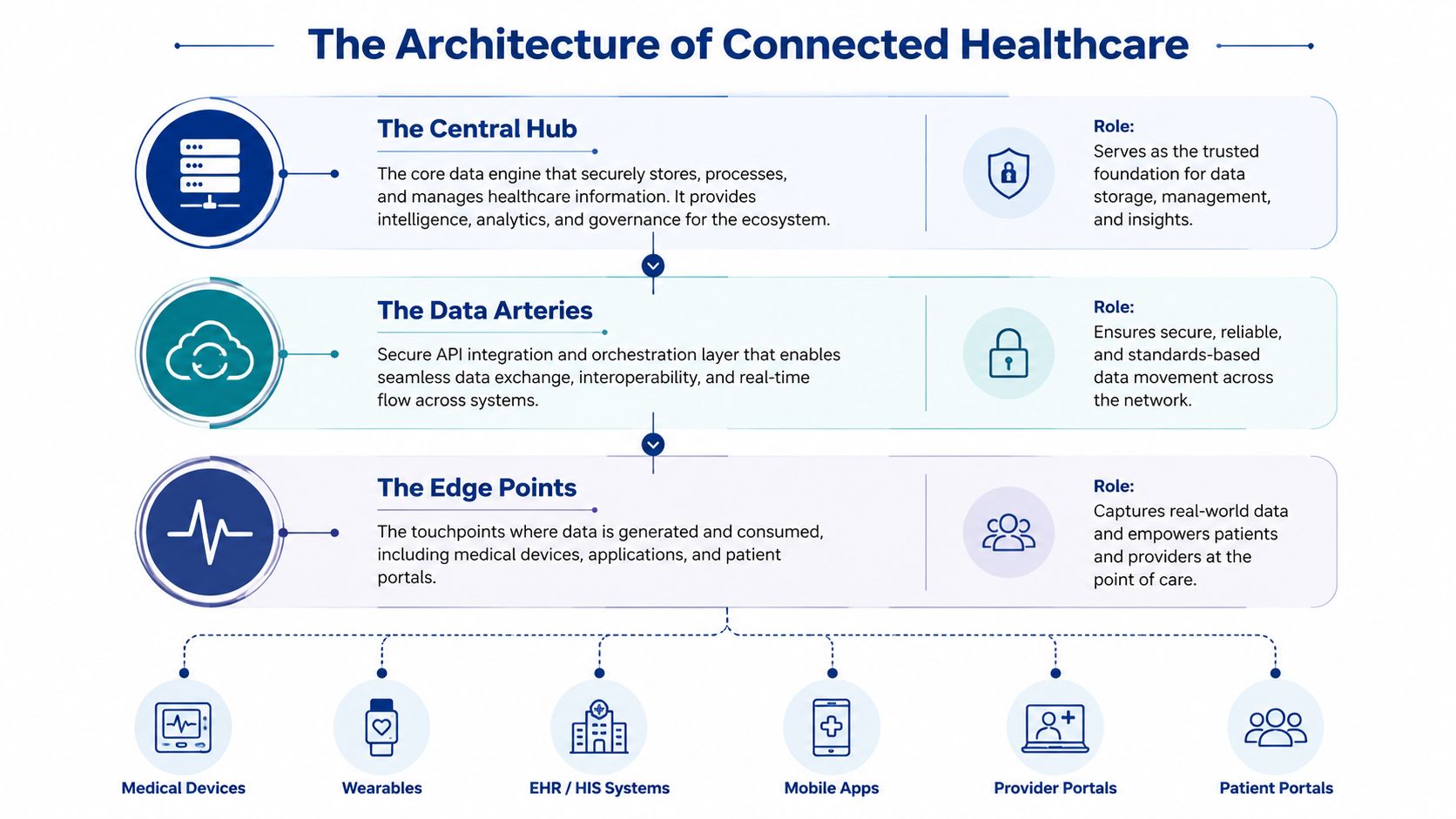
The Central Hub
At the centre sits the core data and workflow engine. The platform receives information from EMRs, scheduling tools, patient apps, billing systems, and connected devices in this central hub. It stores, normalises, and routes that data so it becomes operationally useful rather than just technically available.
A strong platform architecture is modular. That means buyers can start with one capability, such as virtual visits or remote monitoring, then add services without rebuilding the whole stack. According to this market and architecture analysis, the technical benchmark is a modular cloud architecture that aggregates data from multiple device classes, applies analytics, and feeds dashboards, with stronger implementations standardising data at ingestion and exposing it through interoperable APIs.
The Data Arteries
The next layer is integration. These are the secure interfaces, APIs, message brokers, and connectors that let separate systems exchange information. This layer is often where projects succeed or stall.
In real deployments, these are the common stress points:
Patient identity mismatch: One system records a patient differently from another.
Delayed synchronisation: Appointment, device, or medication data arrives too late to be useful.
Custom one-off integrations: Every new interface needs unique maintenance.
Alert overload: The platform ingests data, but routing logic isn't tuned to care pathways.
A buyer should ask whether the vendor has a reusable integration model or whether every connection becomes a bespoke project. The latter gets expensive fast.
The Edge Points
These are the devices and interfaces people touch. Think patient portals, clinician dashboards, tablets in clinics, bedside equipment, home blood pressure cuffs, wearable sensors, and mobile apps.
A useful edge experience has two traits. It feels simple to the user, and it hides substantial complexity underneath. Patients shouldn't need technical support to upload a reading. Clinicians shouldn't click through six screens to review a trend and escalate a case.
Practical rule: Buy architecture for the workflow you'll need in two years, not the demo you saw this week.
A future-proof platform should also account for practical deployment details that administrators often discover too late:
| Architecture concern | What to look for |
|---|---|
| Device connectivity | Secure gateways, support for intermittent connections, edge buffering |
| Scale | Modular services that can expand by site, service line, or patient programme |
| Data quality | Standardised ingestion rules, and validation before data reaches dashboards |
| Operational resilience | Logging, monitoring, auditability, and controlled update processes |
When the architecture is right, every later decision gets easier. When it's wrong, even simple workflow changes turn into long integration projects.
The Crucial Role of Interoperability Standards
A connected healthcare platform is only as useful as its ability to exchange information with the systems you already have. That's why interoperability isn't a technical side note. It's the main buying criterion.
Many vendors claim they integrate. The fundamental question is how. If the answer depends on custom scripts, manual exports, and one-off vendor support, you're buying fragility. If the answer is standards-based exchange with clear data models and documented APIs, you're buying room to grow.
Shared Grammar for Clinical Data
Healthcare systems don't all “speak” the same way. Interoperability standards create a shared grammar so data can move between systems without losing meaning. In practical terms, they help your EMR, patient portal, lab interface, and remote monitoring workflows stay aligned.
The standards most buyers hear about are HL7v2, CDA, and FHIR. They serve different purposes, and they come from different eras of healthcare IT.
| Standard | Primary Use Case | Data Format | Best For |
|---|---|---|---|
| HL7v2 | Messaging between hospital systems | Delimited text messages | Legacy interfaces, admissions, discharges, lab feeds |
| CDA | Structured clinical documents | XML documents | Document exchange, summaries, formal records |
| FHIR | Modern API-based data exchange | Web-friendly resources such as JSON or XML | Cloud platforms, mobile apps, portals, scalable integrations |
Why FHIR Matters More Now
HL7v2 still exists in many environments because hospitals rely on long-established systems. CDA remains useful when document-based exchange is the requirement. But for modern connected healthcare platforms, FHIR is usually the standard buyers should focus on first.
Why? Because it fits how current systems operate. It works well for cloud applications, modular services, patient-facing products, and API-first integration. It also makes it easier to expose smaller, targeted pieces of data, such as medication lists, observations, appointments, or care plans, without sending bulky documents or fragile message formats.
That doesn't mean every organisation can replace older standards overnight. Most real environments are hybrid. A sensible platform should be able to work across old and new patterns while steadily reducing dependence on brittle interfaces.
For a deeper look at what this means in practice, this guide on how FHIR integration transforms healthcare is worth reading before vendor discussions.
Questions Buyers Should Ask Vendors
These questions reveal more than a polished product tour ever will:
How do you use FHIR in production, not just in roadmap slides?
Which resources and workflows are already supported out of the box?
How do you map data from older HL7v2 feeds into your platform?
What happens when our EMR structure doesn't match your default model?
Can another vendor build on top of your APIs later?
If a platform claims to be open but makes every integration dependent on the vendor's services team, that openness is limited.
Interoperability protects you from vendor lock-in. It also protects future projects. New modules, new devices, new reporting needs, and new patient services become manageable when your data foundation speaks a common language.
Integrating IoT and Medical Devices Seamlessly
Connected healthcare platforms become far more valuable when they extend beyond the clinic and into the patient's daily routine. That's where IoT and medical device integration come in. The platform stops being a portal and starts becoming an active part of care delivery.
For Canadian providers, the strongest use case is often chronic disease management. A home reading only matters if it reaches a clinical system, is interpreted in context, and triggers the right action when needed.

From Raw Reading to Clinical Action
A device integration pipeline usually has four jobs:
Capture the reading securely from a home device, wearable, or in-clinic machine.
Normalise the data into a standard format that clinical systems can use.
Match it to the right patient record without ambiguity.
Present it in a workflow context so a clinician or care manager can act.
That sounds straightforward, but execution is where many projects break down. If the data arrives without context, clinicians don't trust it. If alerts fire too often, staff start ignoring them. If patient onboarding is clumsy, the device programme loses participation.
In the Canadian context, connected platforms are justified by the economics of virtual care because they unify remote monitoring device data with clinical systems so clinicians can triage by risk, which is especially important for chronic disease management, where continuous home measurements can be ingested and alerted on in near real time, as outlined in this connected medical devices analysis.
What Works and What Usually Doesn’t
A practical example is a patient managing heart failure at home. Daily weight, blood pressure, and symptom inputs can help a care team identify deterioration earlier than a scheduled review would. But the platform must do more than collect numbers. It has to support threshold logic, escalation rules, and clear responsibility for follow-up.
What tends to work:
Low-friction onboarding: Devices arrive configured, with clear patient instructions.
Clinically tuned alerts: Thresholds reflect local care pathways, not generic defaults.
Dashboard prioritisation: Staff see risk-sorted queues, not endless data tables.
Workflow ownership: Someone knows who contacts the patient and how quickly.
What often fails:
Data without action paths
Too many unsupported device types
Manual reconciliation between the portal and EMR
Remote monitoring programmes with no staffing model
A connected platform should reduce avoidable in-person utilisation when virtual care is integrated into longitudinal patient data and care-team workflows. That's why device integration isn't a gadget strategy. It's a service design problem with technical dependencies.
For healthcare leaders planning device-led care pathways, this article on IoT healthcare solutions for care transformation offers a helpful operational lens.
Device data creates value when the platform sorts signal from noise and places the result inside a clinical workflow someone owns.
The strongest programmes usually start narrowly. One patient group. One care pathway. One escalation model. Then they expand once the workflow proves stable.
Ensuring Security and Regulatory Compliance
Security in connected healthcare platforms can't be treated as a procurement checkbox. It determines whether the platform is deployable, defensible, and trusted by staff and patients. In Canada, that discussion quickly moves to PIPEDA, provincial privacy expectations, and the practical controls needed to handle sensitive health information responsibly.
A platform may have good features and still be the wrong choice if its security model is vague, difficult to audit, or dependent on manual workarounds.

The Controls That Matter in Practice
In healthcare, security has to support operations, not block them. Buyers should look closely at how the platform handles:
Encryption: Protection for data in transit and at rest
Role-based access control: Staff should only see what they need for their role
Audit trails: Every significant access or action should be traceable
Interoperability with safeguards: Integrations must not create privacy blind spots
Canadian deployments also need to account for privacy and interoperability requirements at scale. Connected healthcare environments typically need FHIR or HL7 interfaces, encrypted transport, role-based access control, and auditability to be deployable, especially when remote monitoring and device integrations are involved. That requirement is discussed in the same earlier Canadian technical context, so buyers should treat those controls as baseline expectations rather than premium extras.
Data Residency and Network Realities
For many hospitals, clinics, and health authorities, data residency is a decisive factor. If patient data is stored or processed outside the required jurisdiction, legal and procurement issues can arise before implementation even begins. Buyers should ask where data is stored, where backups reside, and how support access is controlled.
The network itself matters too. A secure platform still depends on stable and properly segmented connectivity across wards, clinics, and device environments. Teams reviewing wireless performance for mobile carts, bedside systems, and connected devices may find useful context in Purple's work on optimising clinical networks for medical devices, especially where coverage gaps affect device reliability.
Security failures in connected care rarely come from one dramatic flaw. They usually come from ordinary gaps such as shared accounts, poor audit visibility, weak onboarding controls, or badly managed integrations.
A practical compliance review should include more than a security questionnaire. It should test the operating model.
Questions Worth Asking Before You Sign
Who can access patient data, and how is that access limited by role?
What audit records are available to administrators?
How are third-party integrations reviewed and monitored?
Where is data stored, processed, and backed up?
How are credentials, support access, and incident response handled?
For teams evaluating build or buy options in regulated environments, this guide to healthcare compliance software development is a useful companion to procurement due diligence.
If a vendor cannot answer these questions clearly, the platform is not ready for a healthcare environment where trust and accountability are essential.
Measuring Your Return on Investment
A connected healthcare platform shouldn't be approved because it sounds modern. It should be approved because it solves a defined operational or clinical problem and because you can measure whether it did.
That's where many projects go wrong. The implementation goes live, usage looks promising, but no one agreed upfront on what success would mean. Then the platform gets judged on anecdote rather than evidence.

Don’t Measure Activity Alone
Buyers increasingly ask whether connected platforms improve efficiency or add integration burden. The answer depends on how well the platform fits EHRs and care workflows, and whether success is measured by meaningful operational outcomes such as reduced no-shows, faster triage, and stronger continuity of care, as noted in this ARPA-H discussion of platform-enabled care delivery.
Visit counts alone won't tell you much. More virtual appointments don't automatically mean better care or lower admin load. A good ROI framework includes three dimensions.
A Practical KPI Framework
| Area | What to measure |
|---|---|
| Clinical value | Care-plan adherence, response time to risk alerts, continuity across care settings |
| Operational efficiency | No-show patterns, triage speed, duplicate data entry, scheduling friction |
| Financial impact | Staff time reallocated, programme scalability, and avoided process waste |
Some results show up quickly. Appointment confirmation workflows, digital intake, and messaging often reduce administrative friction early. Other returns take longer. Remote monitoring value, for example, depends on enough enrolled patients, stable workflows, and clinicians trusting the data.
Where ROI Often Gets Lost
The most common problem isn't the software itself. It's the misalignment between the platform and the operating model.
Watch for these warning signs:
The platform adds clicks because workflows weren't redesigned
Teams receive alerts, but no one owns follow-up
Patient enrolment is too complex for front-desk staff to sustain
Data arrives in dashboards, but not in the clinical record people use
One useful discipline is to create a baseline before implementation. Measure current no-show handling, current staff admin effort, current patient follow-up lag, and current data entry duplication. Then compare after rollout by service line.
The strongest business case for connected healthcare platforms is rarely “more technology”. It's fewer delays, cleaner hand-offs, and better use of clinical time.
ROI becomes visible when the platform removes a real bottleneck. If it doesn't, then the issue may be architecture, workflow design, or scope selection rather than product quality alone.
Making the Right Choice for Your Organisation
The connected healthcare platform market is no longer an emerging niche. It is an established infrastructure. Grand View Research values the global market at USD 16.54 billion in 2025 and forecasts it to reach USD 28.22 billion by 2033, with a 7.06% CAGR from 2026 to 2033, indicating for Canadian buyers that these platforms are becoming core infrastructure and that vendor choice is a strategic decision, according to Grand View Research's connected healthcare platform market report.
That matters because the buying decision now has long-term consequences. Once a platform is connected to your EMR, devices, patient communications, and reporting workflows, replacing it is hard. The right choice is less about brand visibility and more about fit.
What Smaller Clinics and Larger Organisations Should Prioritise
A small clinic usually needs simplicity first. The platform should be easy to adopt, quick to train on, and affordable to operate without a dedicated integration team. If the staff spend more time managing the system than using it, the investment won't hold.
A hospital or multi-site enterprise has different priorities. It needs modular architecture, stronger governance, integration capacity, role-based controls, and room to support multiple service lines. It also needs vendors that can work with legacy realities rather than pretending they don't exist.
A Buyer Checklist That Cuts Through the Sales Pitch
Use these questions during evaluation:
Architecture: Is the platform modular, cloud-based, and able to scale without a rebuild?
Interoperability: How does it support FHIR, HL7, and integration with our existing EMR?
Security and privacy: How does it support PIPEDA-aligned controls, auditability, and data residency needs?
Device strategy: Which remote monitoring and IoT workflows are already proven?
Implementation model: Who handles mapping, migration, testing, training, and support?
Operational impact: Which workflows get easier on day one, and which require redesign?
Exit risk: Can our data and integrations remain usable if we change vendors later?
One practical option for organisations that need custom interfaces around existing systems is to work with an integration partner rather than rely entirely on packaged software defaults. For teams assessing that route, healthcare software integration is the logical area to review, especially when the challenge is connecting established clinical systems with new patient-facing or device-driven services.
The best choice is the one your organisation can operationalise. In connected care, the platform wins only when the workflow works.
If your organisation is weighing connected healthcare platforms and needs a practical route through interoperability, compliance, workflow design, and custom integration, Cleffex Digital Ltd can be explored as a technical partner for building or integrating secure healthcare software in Canadian and North American environments.







