



Most operational leaders in healthcare don't need another dashboard. They need fewer surprises before the morning huddle, fewer bed escalations by midday, and fewer frantic calls about staffing, discharges, and equipment by late afternoon.
That's the daily pattern in many hospitals and clinics. A patient list changes at the last minute. A surgeon finishes early while a downstream unit is backed up. An outpatient session has gaps because some patients don't arrive, while another service line is overloaded. Teams work hard, but they're often working reactively.
Predictive analytics in healthcare operations matters because it changes the timing of decisions. Instead of waiting for a bottleneck to become visible, operations teams can spot the conditions that usually lead to one. Instead of reviewing what happened last week, they can prepare for what is likely to happen next shift, next day, or next discharge cycle.
The tricky part is that providers and software vendors often approach this from opposite sides. Hospital leaders ask whether the model will fit real workflows, protect patient data, and help staff act faster. Product teams ask whether the source data is complete, the integration points are stable, and the model outputs are trustworthy enough to ship into production. Useful systems sit in the middle. They respect clinical operations, and they respect engineering reality.
Beyond the Daily Scramble in Healthcare
A familiar scene plays out across healthcare settings every day. Bed managers are checking capacity while the emergency department keeps filling. Unit leaders are trying to forecast discharges, but the picture changes with every delayed consult, transport issue, or late lab result. Scheduling staff are juggling cancellations in one clinic and long wait lists in another.
The problem isn't a lack of effort. It's that most operational systems were built to record events after they happen. They're good at showing today's census, yesterday's no-shows, or last month's utilisation. They're much less helpful when a hospital needs to know which ward is likely to tighten first, which session is likely to have appointment gaps, or which patients are likely to need more coordination before discharge.
Where reactive operations break down
Reactive operations create a hidden tax on every team.
Front-line staff lose time to manual follow-up, status checks, and workarounds.
Managers make late decisions because the warning signs are buried across several systems.
IT teams get blamed for workflows that were never designed to support forward-looking decisions.
Patients feel the impact through waits, handoff delays, and inconsistent communication.
A lot of organisations already know this. What they need is a practical path out of it. That starts with treating prediction as operational intelligence, not as a science project.
Most failed analytics efforts in healthcare don't fail because the model was weak. They fail because nobody built the step between the prediction and the action.
That's why the operational context matters. A model that predicts likely discharges is only useful if bed control, transport, environmental services, and receiving units can act on it. A no-show prediction only matters if the scheduling rules can adapt without creating new friction for staff.
For leaders working through that transition, this broader view of modern healthcare operations is useful because it frames analytics as part of a connected operating model, not an isolated reporting tool.
What Is Predictive Analytics in Healthcare Operations
Think of predictive analytics as a weather forecast for hospital operations.
Traditional reporting tells you it rained yesterday. You can see that the emergency department was overcrowded, a clinic had unused appointment slots, or a ward discharge target was missed. Predictive analytics asks what conditions are forming now and what they're likely to cause next.
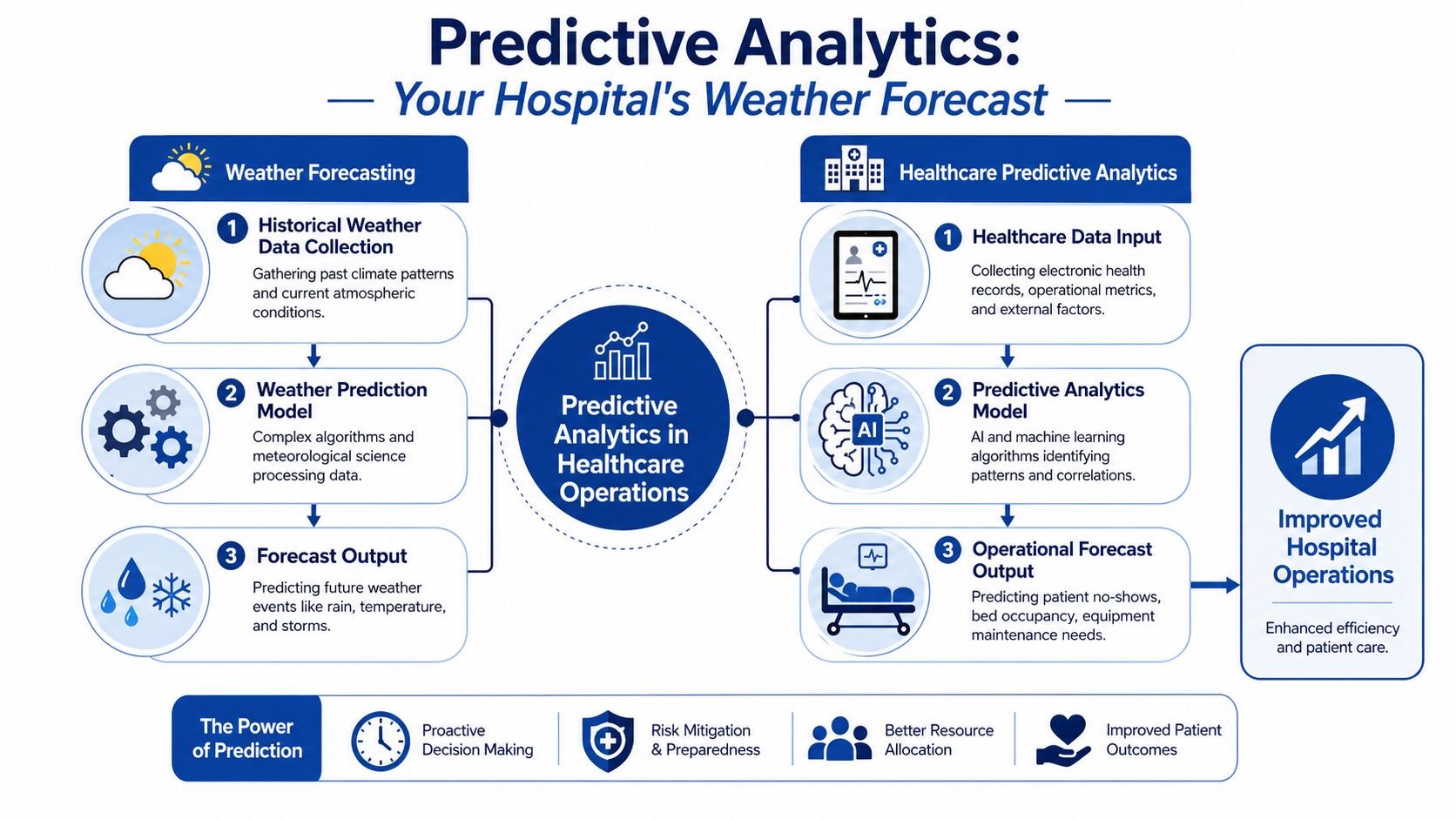
The forecast analogy that actually helps
A weather system works because it combines past patterns with current conditions. Healthcare operations do the same.
A predictive model looks at historical and current signals such as appointment history, discharge timing, staffing patterns, transfer activity, procedure schedules, equipment status, and operational bottlenecks. The model learns which combinations usually lead to a likely outcome. That outcome might be a missed appointment, a delayed discharge, a bed shortage, or a maintenance issue.
Here's the simplest way to separate the main analytics types:
| Analytics type | Core question | Operational example |
|---|---|---|
| Descriptive | What happened? | Yesterday's no-show list |
| Predictive | What's likely to happen? | Patients likely to miss tomorrow's appointments |
| Prescriptive | What should we do? | Hold a reserve slot or trigger reminder outreach |
The middle layer is the one many providers miss. They either stay with reporting, or they jump straight to automation without a reliable forecast in between.
What the model actually produces
In practice, a predictive tool usually doesn't produce magic. It produces something plain and usable:
A risk score for likely no-shows or readmissions
A forecast curve for likely admissions or bed demand
A priority list for likely discharge blockers
A maintenance alert for equipment with failure patterns
That simplicity matters. Operational users don't need to inspect model architecture during a shift. They need output that fits decisions they already make.
Practical rule: If a manager can't explain the model output in one sentence, the implementation is probably too abstract for day-to-day use.
From the vendor side, that means building not just the model, but also the interpretation layer. Good teams spend as much time on labels, thresholds, workflow triggers, and exception handling as they do on feature engineering.
Key Applications Transforming Hospital Workflows
The strongest use cases for predictive analytics in healthcare operations are rarely the flashiest ones. They're the places where small delays multiply across teams and where better timing improves both throughput and staff experience.
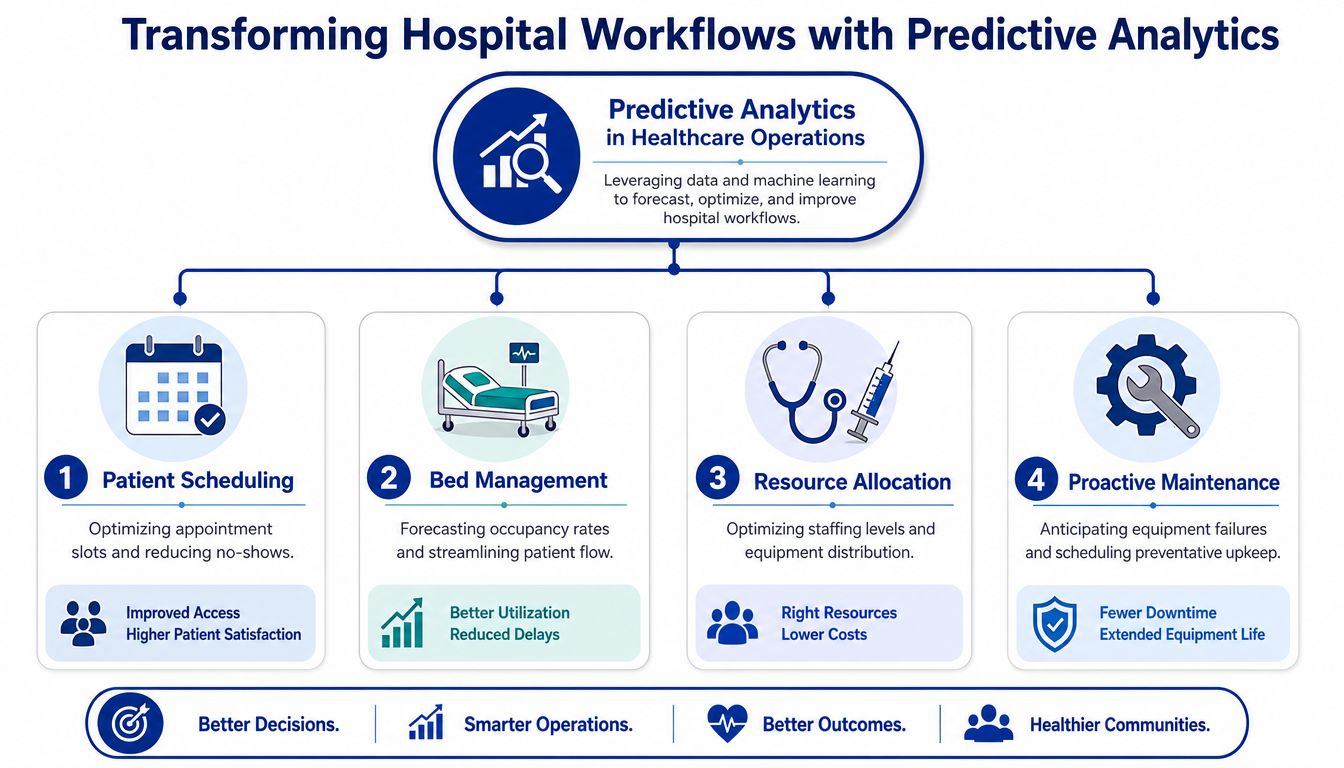
Patient scheduling
Most scheduling teams already know which sessions are fragile. They know certain appointment types run late, some patients need extra follow-up, and some clinics experience repeated no-shows. Predictive models make that knowledge systematic.
A useful scheduling model might combine appointment history, booking lead time, channel of confirmation, visit type, and local operational patterns. The output can support reminder prioritisation, wait-list activation, or careful overbooking in tightly controlled settings.
What doesn't work is treating no-show prediction as an isolated probability score. If the scheduling software can't route follow-up tasks or offer replacement slots quickly, the forecast stays interesting but operationally weak.
Bed management
Bed flow is one of the clearest examples of where a good forecast beats a heroic response. Operations teams need to know more than current occupancy. They need a realistic view of likely discharges, pending transfers, expected admissions, and delays in bed turnaround.
A practical model often brings together ADT feeds, procedure schedules, discharge planning status, transport requests, and unit-specific patterns. The value isn't only in predicting bed pressure. It's in helping teams sequence actions earlier.
A simple comparison shows the shift:
| Before prediction | After prediction |
|---|---|
| Staff react to shortages after units tighten | Teams prepare for likely pinch points earlier |
| Bed meetings focus on current status only | Bed meetings include likely next-step demand |
| Discharge delays surface late | Likely blockers surface while there's still time to act |
Readmission and follow-up risk
Readmission is often discussed as a clinical quality issue, but it also has an operational side. Follow-up access, care coordination, medication reconciliation, and discharge communication all affect what happens after a patient leaves.
The best operational models don't pretend to replace clinical judgement. They identify patients who may need more deliberate discharge planning, earlier follow-up booking, or outreach coordination. That makes the model valuable to care managers and operations leads at the same time.
This is also where adjacent tools matter. If your organisation is exploring patient communication workflows, this overview of how AI chatbots help medical teams is relevant because conversational tools can support reminders, triage, and follow-up pathways around predictive triggers.
Supply chain and maintenance
Hospitals don't only run on clinicians and beds. They run on equipment availability, replenishment timing, and dependable support services. Predictive methods can flag likely stock pressure, identify usage patterns that drive shortages, and anticipate maintenance windows before equipment failure disrupts care.
Vendors often underestimate this area because the workflow spans biomed, facilities, procurement, and clinical users. Providers underestimate it because the gains feel less visible than patient-facing use cases. In practice, it's one of the cleaner places to prove value because operational actions are often easier to define.
Building Your Predictive Model Data and Tools
A predictive model is only as useful as the data and delivery stack behind it. In healthcare, that means the fundamental work starts long before anyone chooses an algorithm.
Start with the data you already trust
Most organisations don't need exotic data to begin. They need better use of existing operational data.
Common inputs include:
EHR and ADT records for patient movement, encounter status, and discharge patterns
Scheduling systems for appointment history, cancellations, booking windows, and clinic templates
Administrative data for staffing rosters, room allocation, and service line activity
Device and equipment feeds for utilisation and maintenance signals
External context such as weather, public holidays, or local event calendars when those factors affect demand
The trap is assuming those sources are ready. They usually aren't. Time stamps conflict. Status fields are used inconsistently. Different departments define the same event in different ways. A vendor can build a competent model and still fail because “discharge ready” means one thing in the nursing workflow and another thing in the reporting layer.
Clean labels beat fancy models. If your historical outcome data is inconsistent, the model will learn your process noise along with your real operational patterns.
Choose tools that match the maturity of the team
The technical stack should match the organisation's capacity to maintain it. That usually means a data platform, an integration layer, a model development environment, and a delivery mechanism inside the workflow.
For some teams, a cloud warehouse and a managed machine learning platform are enough. For others, especially those dealing with fragmented source systems, the harder problem is ingestion, transformation, and governance. If your team is evaluating modern data platforms, it helps to explore Databricks solutions on DataEngineeringCompanies.com because much of the implementation burden sits in data engineering rather than in model training.
A few model categories cover most operational use cases:
Classification models for yes-or-no style risks such as no-show likelihood
Regression models for forecasting counts, durations, or demand
Time-series approaches for repeating patterns across shifts, days, or seasons
Anomaly detection for identifying equipment or workflow behaviour that deviates from normal
One practical market option in this space is Cleffex Digital Ltd, which offers operational AI solutions for functions such as patient scheduling and bed management. The main selection criterion shouldn't be branding. It should be whether the tool fits your source systems, governance requirements, and workflow design.
A Practical Roadmap for Implementation
The safest way to adopt predictive analytics is to treat it like an operational change programme with software attached, not a software project with operations attached.
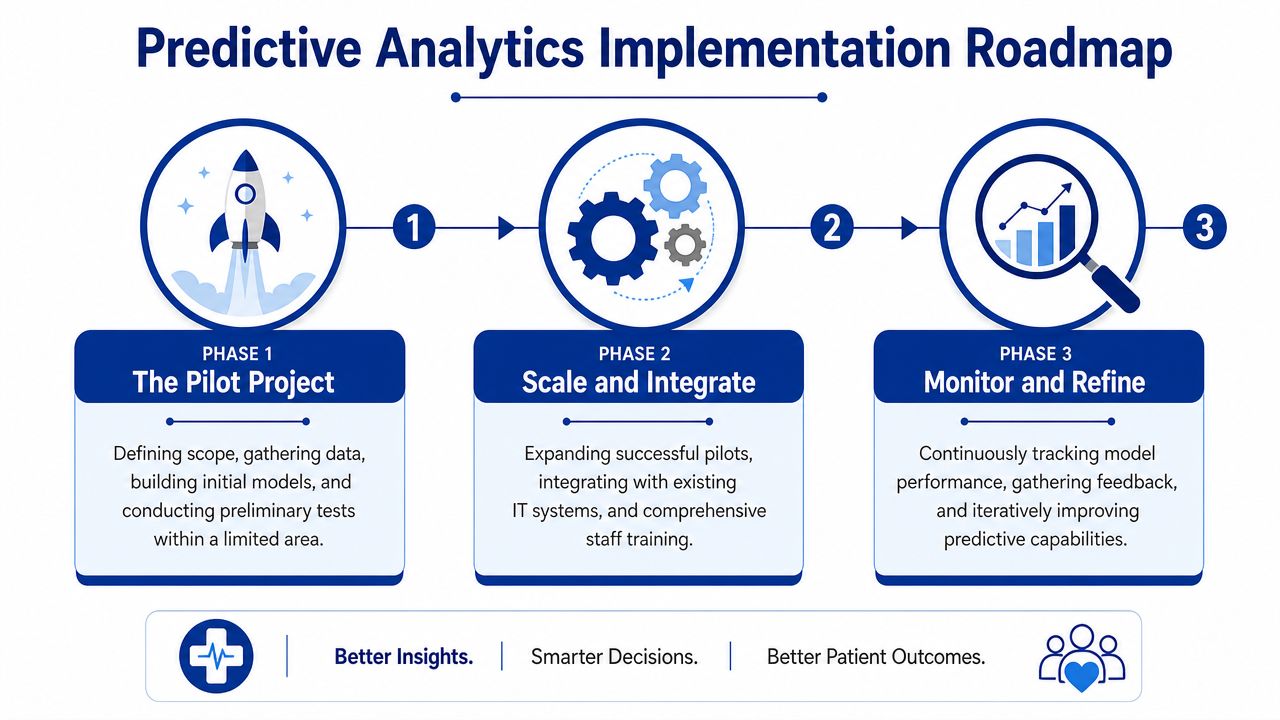
Phase one with a tightly scoped pilot
Start with one problem that is painful, frequent, and measurable. Good early candidates include outpatient no-shows, discharge timing, or procedure schedule slippage in a single service area.
A disciplined pilot has a few traits:
A named operational owner who feels the problem every week
A clear action path after each prediction
A contained data footprint that doesn't depend on ten systems at once
A review cycle where staff can challenge outputs and improve usability
Many vendors overbuild. They try to create a flexible enterprise platform before proving one narrow workflow. Providers do the reverse. They approve a pilot but don't assign enough operational ownership. Both mistakes create drift.
Phase two by refining what staff will actually use
Once the pilot works, the next step isn't immediate scale. It's refinement.
Review where users ignored the prediction, where they trusted it too much, and where the workflow created extra clicks or duplicate effort. Then adjust thresholds, interface design, alert timing, and escalation rules. A mediocre model inside a clean workflow usually outperforms a stronger model buried in a clumsy screen.
Here's a practical sequence:
Validate the prediction quality against real operational outcomes.
Test intervention rules so staff know what action follows each output.
Retire manual workarounds that duplicate the new process.
Expand carefully to similar departments, not every department at once.
Phase three through enterprise integration
The long-term value comes when predictive outputs appear inside the systems people already use. That may be the EHR, bed board, scheduling interface, command centre view, or an operational work queue.
For many healthcare organisations, that broader integration journey overlaps with larger platform decisions. This discussion of connected healthcare platforms is relevant because predictive tools rarely succeed when they remain detached from the rest of the digital environment.
The model doesn't need centre stage. The workflow does. If staff must leave their normal system to find the prediction, adoption usually fades.
From the vendor side, this phase sees integration engineering, permissioning, auditability, and uptime become more important than data science novelty. From the provider side, at this stage, change management becomes real because model output starts affecting bed calls, booking decisions, and follow-up tasks across teams.
Navigating Compliance and Measuring ROI
Executives usually ask two questions before predictive analytics moves beyond a pilot: is it compliant, and is it worth the operational investment? Those are the right questions.
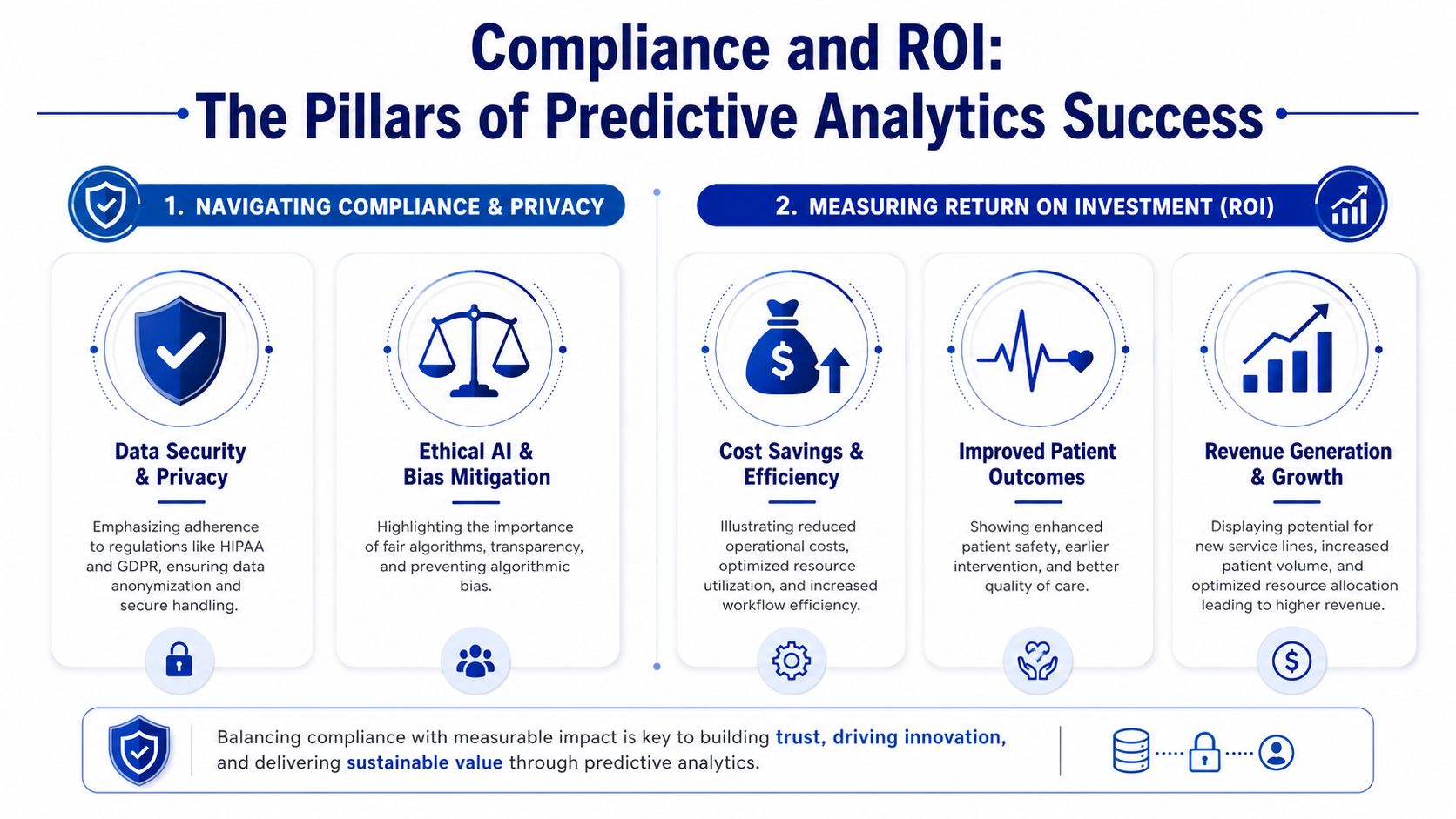
Compliance isn't a final review step
In Canada, organisations need to think seriously about privacy obligations such as PIPEDA. In the United States, HIPAA shapes how protected health information is handled. In both settings, predictive programmes need governance from the start, not after a vendor demo succeeds.
That means reviewing:
Data minimisation so teams only use what the model needs
Access control so operational forecasts don't become broad data exposure
Auditability so teams can trace who saw what and when
Bias review so predictions don't subtly reinforce uneven treatment
Explainability so staff can understand why a risk flag exists
If your team is formalising controls around vendor handling, hosting, and operational safeguards, this guide to healthcare SOC 2 audits can help frame what external assurance work often looks like. Broader security architecture also matters, especially where analytics pipelines connect with clinical systems, and this piece on data security in healthcare information systems fits that discussion.
ROI should be measured at the workflow level
A weak business case talks about AI in broad terms. A strong one ties value to a specific operational decision.
Use-case by use-case, ask four things:
| Question | What to look for |
|---|---|
| What process changed | Scheduling, bed turnover, discharge planning, maintenance routing |
| Who acts on the prediction | Clerk, charge nurse, flow manager, care coordinator, biomed team |
| What metric should move | Wait times, unused slots, bed delays, staff rework, equipment downtime |
| What cost or capacity impact follows | Fewer disruptions, better utilisation, more consistent throughput |
Measure the baseline before rollout. Then compare the post-implementation workflow, not just the model output. If staff received risk scores but nothing changed operationally, there isn't real ROI yet.
A prediction has no business value by itself. Value appears only when a team changes a decision, a timing point, or a workflow branch.
That sounds obvious, but it's where many programmes get stuck. Leadership sees a technically successful pilot, while front-line teams see another screen. The organisations that realise value make the operational change explicit.
Becoming a Future-Ready Healthcare Organisation
The organisations that get the most from predictive analytics don't treat it as a bolt-on intelligence layer. They treat it as part of how the operation learns.
That shift matters. Hospitals and clinics won't eliminate uncertainty. Patient demand changes, staffing pressures remain, and care pathways don't behave like factory lines. But they can reduce avoidable surprises. They can identify likely congestion before it locks up a unit. They can move from broad staffing guesses to more informed planning. They can make scheduling, bed flow, discharge, and maintenance less dependent on last-minute heroics.
What future-ready actually looks like
A future-ready healthcare organisation usually shows a few clear habits:
Operations and IT share ownership of the use case instead of handing work across a wall.
Vendors design for workflow reality rather than shipping models that look impressive in isolation.
Clinical and operational leaders challenge predictions and improve them over time.
Governance, privacy, and usability are built in early, not patched in later.
The bridge between clinic and code is where most of the value sits. Providers know the friction points that matter. Software teams know how to turn scattered system data into usable signals. When those perspectives work together, predictive analytics in healthcare operations becomes practical instead of aspirational.
Healthcare leaders don't need to transform everything at once. They need one credible use case, one workflow that improves, and one team that trusts the result enough to keep going.
Cleffex Digital Ltd works with organisations that need secure, custom healthcare software and operational AI capabilities, including systems that support scheduling, workflow automation, and platform integration. If you're evaluating predictive analytics in healthcare operations and need a partner that can bridge practical care delivery needs with software development execution, learn more at Cleffex Digital Ltd.







