



Canadian healthcare leaders don't need another abstract AI debate. They need to know whether the technology can solve real operating problems inside a regulated, resource-constrained system. One number changes the frame immediately: 12.2% of businesses in Canada reported using AI to produce goods or deliver services in the preceding 12 months in Q2 2025, up from 6.1% in Q2 2024, according to Statistics Canada. In healthcare, the pace has been even sharper, with the share of organisations that adopted or explored generative AI rising from 72% in Q1 2024 to 85% by the end of the year in that same source.
That matters because medical AI solutions are no longer side projects for innovation teams. They're becoming operating tools for radiology, nursing, administration, patient access, and clinical governance. The question isn't whether AI belongs in Canadian healthcare. It's where to apply it first, how to manage risk, and how to prove value without creating a compliance problem.
The New Frontier of Healthcare Medical AI Solutions
AI has moved from pilot language to boardroom language. Canadian organisations are adopting it because labour pressure, documentation burden, fragmented workflows, and rising care demand are forcing leaders to look for effective solutions.
Healthcare sits at the centre of that shift. It generates large volumes of clinical text, imaging, scheduling data, supply data, and administrative work. Those are exactly the kinds of environments where software can assist people by sorting, summarising, flagging, and prioritising.
What makes this a new frontier isn't that machines are replacing clinicians. They aren't. The practical model is augmentation. A physician still diagnoses. A nurse still triages. A radiologist still signs off. AI helps them get to the right information faster and reduces the amount of low-value manual effort wrapped around clinical work.
Three realities are driving interest in medical AI solutions across Canada:
Operational pressure: Teams need help managing documentation, scheduling, and throughput.
Clinical complexity: Clinicians are working with more data than any one person can manually review in real time.
Governance pressure: Boards want innovation, but they also need defensible controls, privacy discipline, and measurable outcomes.
AI in healthcare works best when leaders treat it as workflow redesign supported by software, not as software searching for a problem.
That's why the strongest use cases tend to be narrow and concrete. Reduce reporting delays in imaging. Improve deterioration alerts for inpatients. Automate parts of medical documentation. Identify likely trial candidates from unstructured notes. Support capacity planning.
Medical AI solutions become useful when they solve one expensive bottleneck at a time.
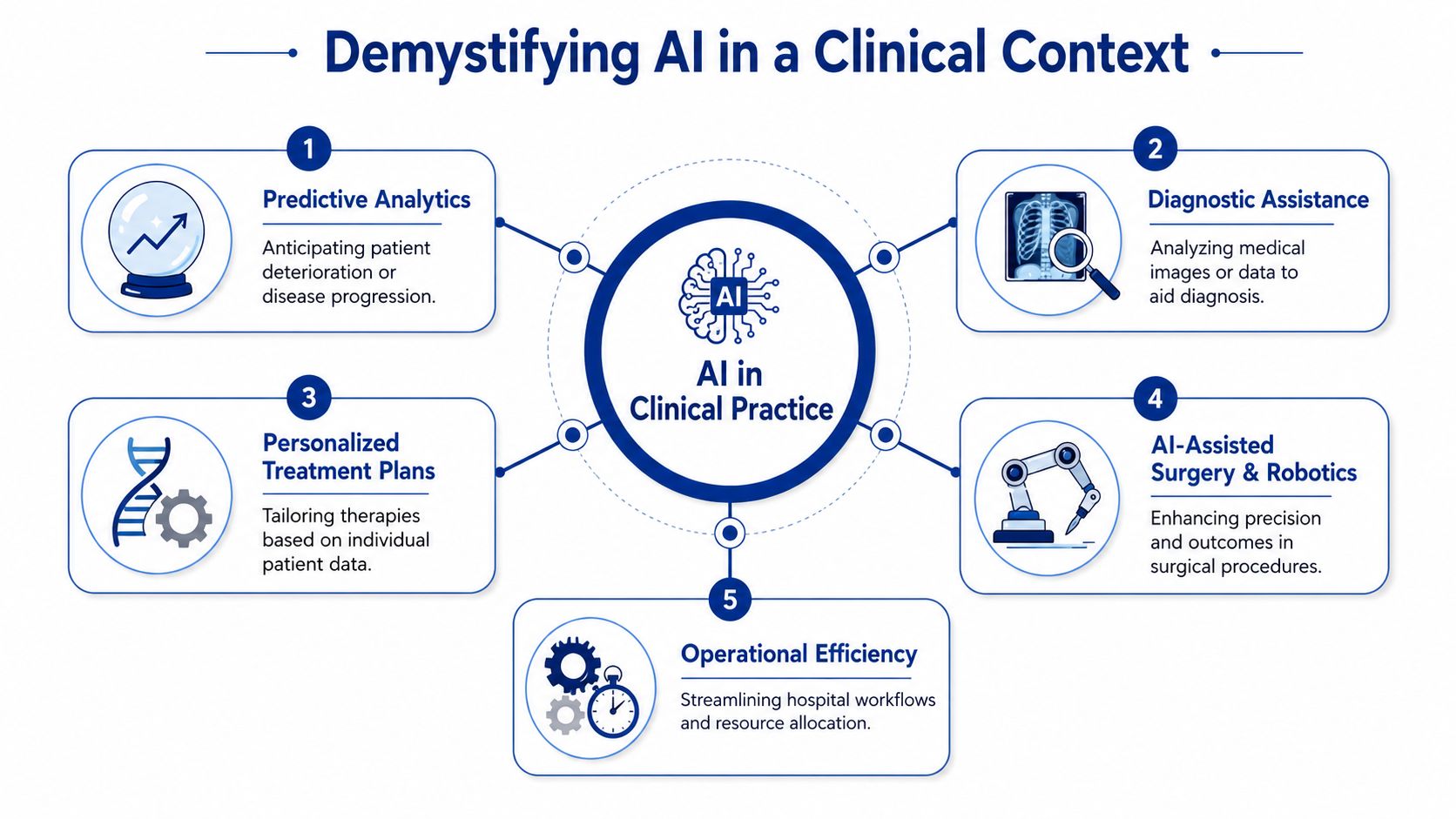
Demystifying AI in a Clinical Context
In a hospital, AI is easiest to understand if you think of it as a super-powered medical assistant. Not an independent clinician. Not a robotic replacement. An assistant that can read fast, recognise patterns, and handle repetitive digital tasks at scale.
What the main AI terms mean in plain language
Machine learning means software learns from examples. In practice, that could mean reviewing past patient records to help spot which combination of signs tends to precede deterioration.
Deep learning is a more specialised form often used for complex pattern recognition, especially in images. That's why it shows up so often in radiology and diagnostics.
Natural language processing, often shortened to NLP, means software can work with human language. In healthcare, that usually means reading notes, extracting key facts, summarising visits, or turning conversation into structured documentation.
A simple way to think about the division of labour is this:
| AI capability | What it does in care settings | Human role |
|---|---|---|
| Pattern detection | Finds signals in data that are easy to miss manually | Clinician interprets relevance |
| Language handling | Summarises notes and extracts details from records | Staff verify and use the output |
| Prediction support | Flags risk of deterioration or workflow issues | Teams decide how to respond |
The job AI is hired to do
Medical AI solutions usually fall into one of two jobs.
First, they help with clinical signal detection. A system reviews data and points people to something important, such as a suspicious image, a rising risk score, or a likely care gap.
Second, they help with workflow compression. They reduce the time between work entering the system and work being completed. That could mean faster chart summarisation, easier referral handling, or quicker document generation.
Health Canada's guidance gives practical examples of both. It notes that AI scribes can use NLP to extract data from unstructured records to identify patients suited for clinical trials, and that AI-powered clinical decision support can forecast deterioration risk in hospitalised patients, enabling earlier intervention. Those examples matter because they show AI acting as support around care, not as unsupervised care itself.
For teams exploring more advanced orchestration, resources on configuring AI experts with LLMs can help clarify how different AI roles can be structured safely around specialised tasks.
Practical rule: if you can't describe the AI's job in one sentence, the use case is probably still too vague to implement well.
Confusion usually starts when organisations buy into broad promises. The safer path is to ask a narrower question: what piece of work is costly, repetitive, delay-prone, and data-rich? That's where AI usually earns its place.
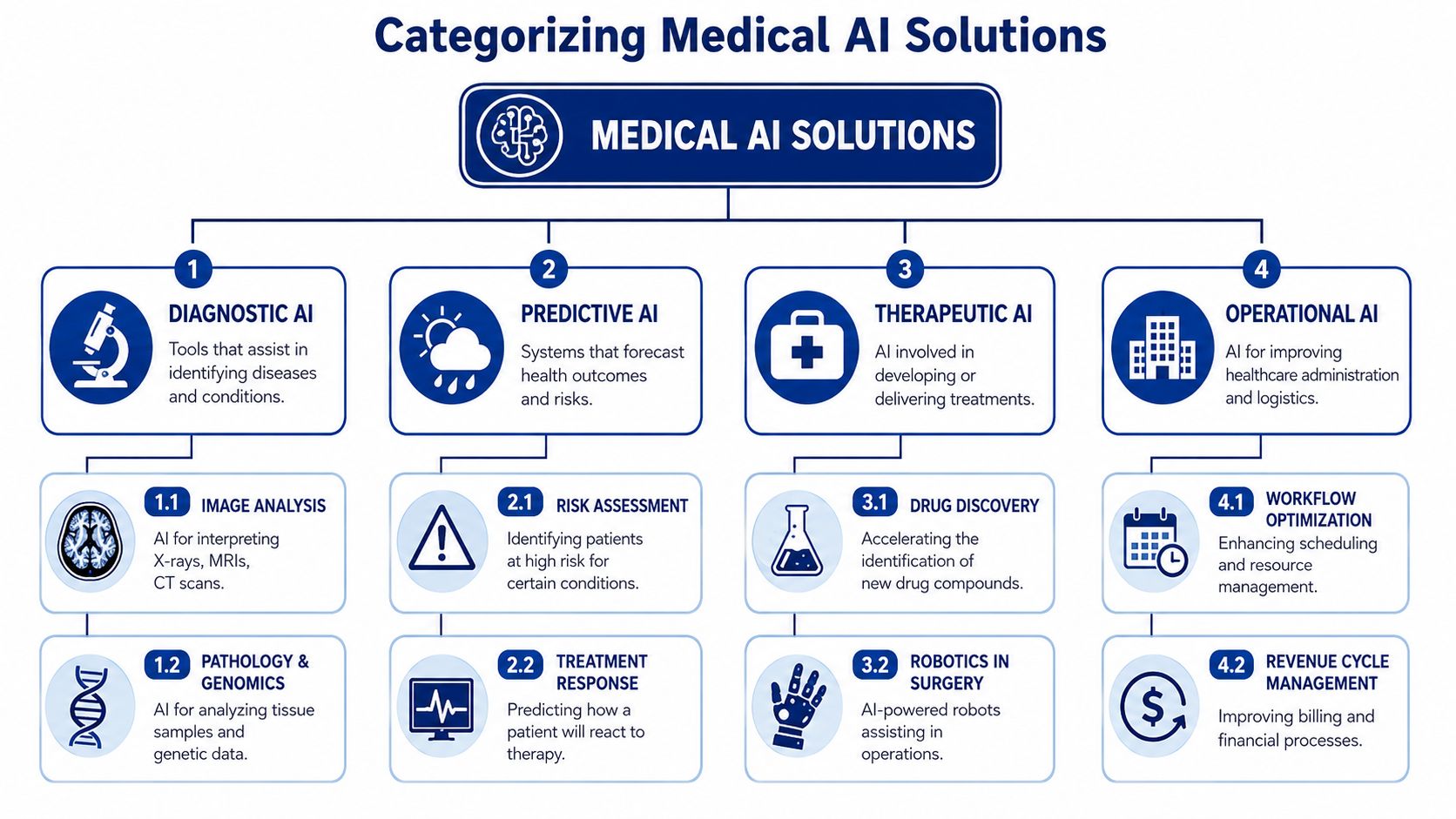
Categorising the Tools Transforming Patient Care
The medical AI market in Canada has already reached USD 224.1 million in 2025 and is projected to reach USD 3,321.44 million by 2033, according to IMARC Group's analysis of the Canadian artificial intelligence in healthcare market. That scale reflects a broad toolset, not one product category.
Diagnostic imaging analysis
This is the most mature category in many organisations. Radiology accounts for over 70% of FDA-cleared AI medical devices in the same IMARC source, largely because image-heavy workflows fit AI well. Deep learning systems can review X-rays and CT scans for patterns linked to tumours, fractures, or bleeds.
That doesn't remove the radiologist. It changes the queue. Cases can be prioritised, suspicious findings can be flagged sooner, and review time can be used more intelligently. For leaders comparing use cases, this is why imaging often becomes the first serious conversation. A detailed overview of this category appears in Cleffex's article on AI for medical imaging and diagnostics.
Predictive analytics
Predictive systems look forward rather than just reading what already happened. They analyse current and historical data to estimate what may happen next, such as deterioration risk, likely complications, or resource demand.
In operational terms, this helps teams move from reacting late to intervening earlier. For an inpatient unit, that might mean extra attention on a patient whose data suggests worsening status. For management, it could mean better bed planning or supply coordination.
NLP for clinical and administrative work
This is the category many executives underestimate because the output can look simple. Yet it's often where the time burden sits. NLP tools can review dictated notes, convert conversations into draft summaries, pull key fields from unstructured text, and support documentation-heavy processes.
One useful way to think about it is that NLP turns scattered language into usable workflow inputs. In fertility and reproductive care, for example, AI is also being applied to image and pattern review in ways that complement specialist judgement.
Remote monitoring and patient follow-up
Some medical AI solutions watch streams of patient data coming from devices, home monitoring tools, or follow-up systems. Their role is to identify who may need attention first.
This category is especially helpful when care teams must track many patients at once and can't manually review every signal with equal depth. The software acts like a triage layer for digital care.
Clinical workflow automation
Not every high-value AI use case is diagnostic. Some of the best returns come from fixing movement through the system. Workflow automation can support scheduling, document routing, referral processing, coding assistance, and internal task coordination.
A quick comparison helps boards sort these categories:
| Category | Primary purpose | Example outcome |
|---|---|---|
| Diagnostic AI | Support clinical interpretation | Faster review of imaging findings |
| Predictive AI | Forecast risk or demand | Earlier escalation for vulnerable patients |
| NLP tools | Structure and summarise text | Less manual documentation burden |
| Remote monitoring | Prioritise follow-up | Faster response to concerning signals |
| Workflow automation | Reduce process friction | Smoother scheduling and task flow |
The point isn't to buy one of everything. It's to match the category to the bottleneck.
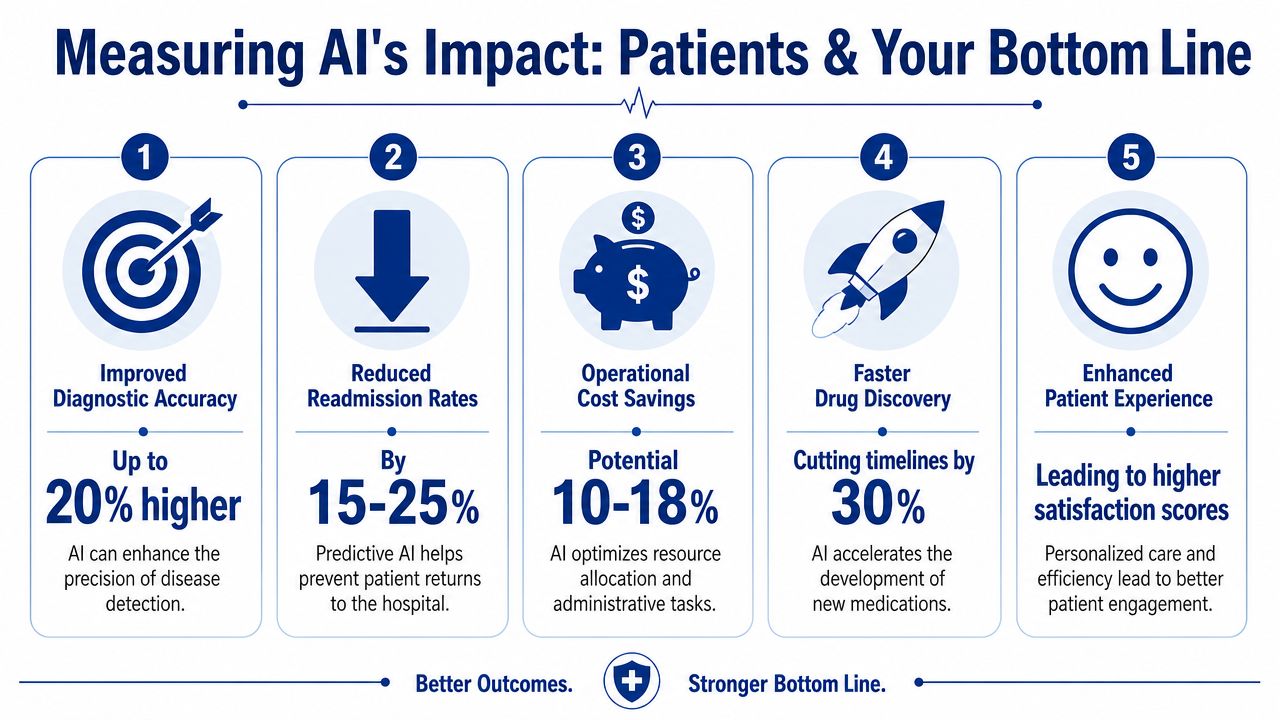
Measuring the Impact on Patients and Your Bottom Line
The strongest financial case for medical AI solutions in Canada isn't theoretical. A McKinsey analysis found that full-scale deployment of known AI applications could reduce Canada's net healthcare spending by approximately 4.5% to 8.0% annually, or CA $14 billion to CA $26 billion per year, and that automated medical documentation alone could generate CA $5 billion to CA $9 billion in net savings, according to McKinsey's healthcare AI analysis for Canada.
Where value shows up first
Boards often ask for ROI as if AI has one universal formula. It doesn't. Value appears in different places depending on the use case.
For a radiology leader, value may show up as shorter time from image acquisition to report prioritisation. For a chief nursing executive, it may show up as earlier warning on patient deterioration. For a CFO, it may appear in documentation efficiency, better capacity use, and lower administrative burden.
A practical lens is to track impact across two dimensions:
Patient impact: Speed, safety, timeliness, consistency
Business impact: Labour use, throughput, avoidable delay, affordability
The patient story behind the business case
Consider a patient with a possible intracranial haemorrhage. When imaging review and reporting happen faster, decisions about escalation can happen faster too. The IMARC source notes that post-AI implementation in Canada, clinical studies showed reduced time from scan to radiologist report for intracranial haemorrhage cases, leading to faster neurosurgical interventions and a statistically significant decrease in 30-day mortality rates.
That's a useful reminder that workflow speed isn't just an operations metric. In acute care, time changes outcomes.
Now consider a different scenario. A clinician finishes a long shift and still has charting to complete. AI-supported documentation doesn't diagnose the patient, but it can reduce the after-hours clerical load. That matters because the organisation benefits twice. Staff time is used more effectively, and clinicians get more room to focus on direct care.
Better healthcare economics and better patient care often come from the same change. Remove friction from the workflow, and people can spend more time on the part only humans should do.
What boards should ask vendors and internal teams
A good impact discussion is specific. Not "Will AI help us?" but questions like these:
Which delay are we reducing?
Report turnaround, note completion, trial matching, bed planning, or something else.
Which decision gets better?
Escalation, diagnosis support, scheduling, coding, or resource allocation.
Which team feels the improvement first?
Radiology, nursing, admin staff, physicians, or patient access.
How will we know the tool is helping rather than merely adding another screen?
A small scorecard keeps the conversation grounded:
| Outcome area | What to watch |
|---|---|
| Clinical timeliness | Whether teams can act sooner on urgent cases |
| Documentation burden | Whether staff spend less time on manual text handling |
| Operational flow | Whether queues, handoffs, or bottlenecks ease |
| Care quality | Whether clinicians trust and use the outputs appropriately |
If you can't tie the proposed tool to one of those lines, the business case usually isn't mature enough.
Meeting Compliance and Data Security Requirements
In Canadian healthcare, an AI project can look promising in a demo and still fail in procurement, privacy review, or clinical governance. That's because adoption isn't just a technology decision. It's a trust decision.
The three checks before you scale
The first check is data quality. If the source data is incomplete, inconsistently labelled, or pulled from workflows that don't reflect actual practice, the model won't perform as intended. Teams need to know what data is being used, how it was selected, and whether the training and validation conditions match the care environment where the tool will run.
The second check is regulatory fit. Health Canada requires machine learning-enabled medical devices to follow lifecycle management across data selection, design, risk management, clinical validation, and post-market monitoring. It also explicitly requires Sex and Gender-Based Analysis Plus so that systems are assessed for equitable performance across under-represented groups, as set out in Health Canada's pre-market guidance for machine learning-enabled medical devices.
The third check is technical validation within actual workflow. A model can perform well in a controlled setting and still create problems when inserted into daily care. Alerts may come at the wrong time. Interfaces may slow staff down. Outputs may be technically accurate but clinically awkward.
How PIPEDA and practical privacy governance fit in
For many leaders, privacy concern starts with a simple question: where is the patient data going, and who can access it? In Canada, that concern often sits alongside PIPEDA obligations and additional sector or provincial rules. The operational response isn't hand-waving about encryption. It's disciplined governance over collection, use, access, retention, auditability, and vendor accountability.
A useful reference point is this Cleffex guide on AI in healthcare data privacy in Canada, which outlines the kinds of privacy and security questions teams should resolve before deployment.
Healthcare organisations should also examine adjacent service models, not just core clinical AI. For instance, if your patient communication workflows involve AI-assisted intake or support, this guide for healthcare call services is a useful operational comparison for thinking through compliant handling of sensitive information in service interactions.
A compliant AI system isn't just accurate. It's governable. Your team must be able to explain what it does, what data it uses, and what happens when it's wrong.
A board-level checklist
Rather than treating compliance as a legal appendix, put it into project gates:
Define the system role clearly: Is it support software, workflow software, or a regulated device-related function?
Document validation logic: What evidence shows it works in your patient population and care context?
Test fairness explicitly: How will performance be reviewed across patient subgroups?
Set post-launch monitoring: Who watches for drift, errors, complaints, or misuse?
Clarify vendor responsibilities: Who updates the model, who logs incidents, and who owns corrective action?
Here, many AI projects become real. Or stop.
Your Step-by-Step Guide to Adopting Medical AI
The safest way to adopt medical AI solutions is to treat them like any other high-stakes clinical transformation. Start with a narrow problem, validate in a controlled setting, then scale only after the workflow and governance hold up.
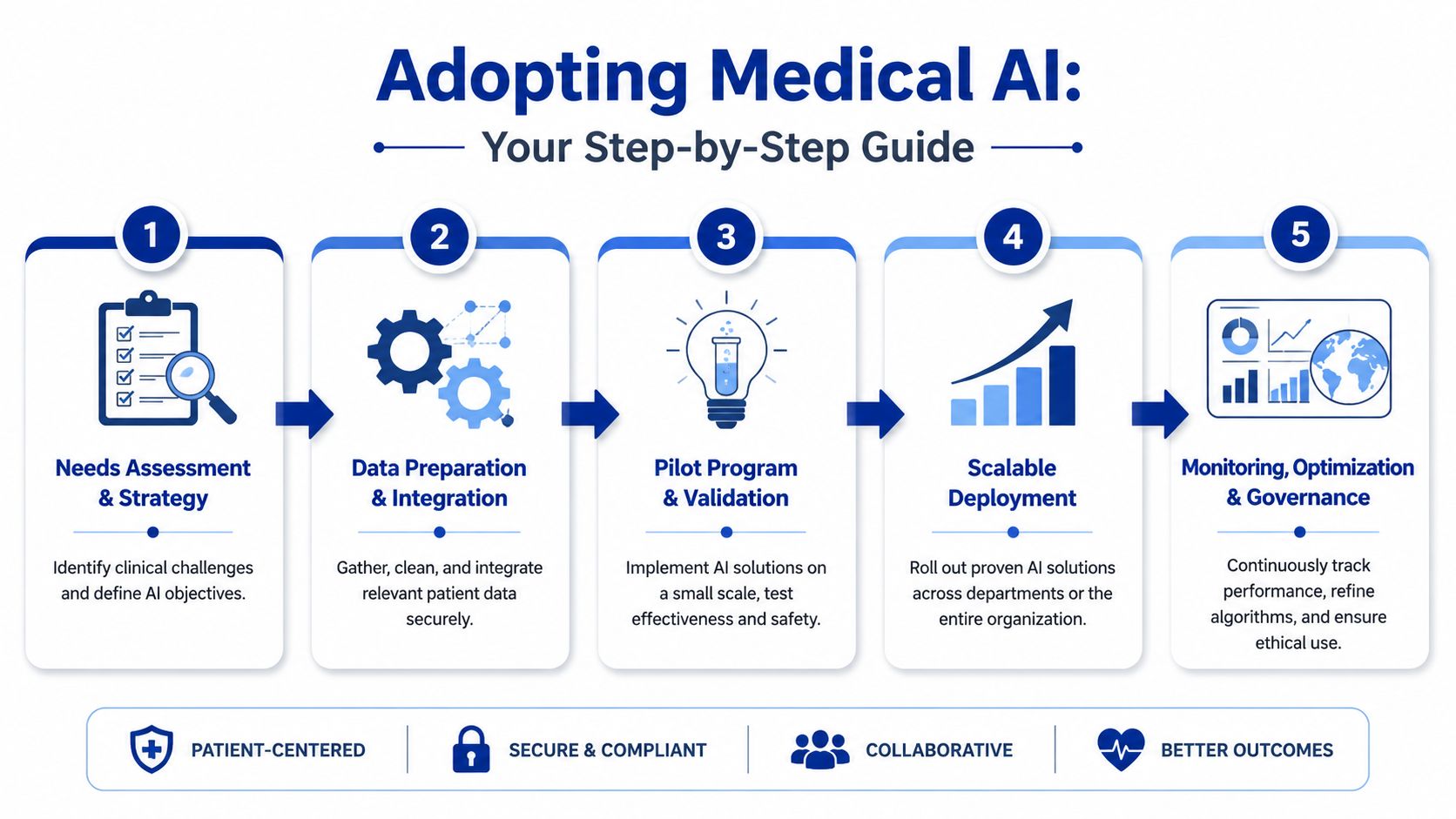
Step 1 and 2: Define the problem and prepare the data
Most organisations begin too wide. "We want AI" is not a project brief. A good starting point sounds more like this: "We need to reduce turnaround delays in one imaging workflow," or "We need better support for documentation in one clinic."
Then prepare the environment around that use case.
Choose one costly bottleneck: Focus on a problem with visible operational pain and a clear owner.
Map the current workflow: Identify where data enters, who acts on it, and where delays occur.
Check data readiness: Confirm that the relevant records, notes, images, or operational data are accessible and usable.
If your organisation is still maturing its broader adoption posture, Cleffex's piece on AI adoption in Canadian enterprises is a useful way to frame internal readiness beyond the healthcare department alone.
Step 3: Run a pilot that can actually be judged
A pilot should be small enough to govern and specific enough to evaluate. That usually means one department, one workflow, and one set of accountable stakeholders.
Good pilots have these traits:
| Pilot element | What good looks like |
|---|---|
| Scope | One narrow clinical or administrative use case |
| Ownership | Clear clinical, operational, and technical leads |
| Success criteria | Defined before launch, not after |
| Fallback plan | Staff can continue safely if the tool underperforms |
Don't ask the pilot to prove everything. Ask it to answer a limited set of operational questions. Does the tool fit the workflow? Do staff trust it enough to use it? Does it reduce a known pain point without creating new risk?
Step 4 and 5: Select partners carefully and scale with governance
Vendor selection is where many organisations either de-risk the initiative or import future trouble. Ask vendors to show how they validate outputs, support auditability, and fit Canadian healthcare compliance expectations. If the answer is mostly marketing language, keep looking.
One option in the market is Cleffex Digital Ltd, which builds custom software and AI-driven solutions for healthcare and life sciences organisations where integration, workflow fit, and compliance planning matter alongside functionality. That's relevant when an off-the-shelf product doesn't align with your systems or process design.
When you're ready to scale, do it deliberately:
Integrate with existing systems carefully: EHR fit, identity management, and workflow timing matter more than interface polish.
Train users on limits, not just features: Staff need to know when to rely on the tool, when to override it, and how to report issues.
Create a standing governance loop: Review performance, user feedback, fairness concerns, and operational impact continuously.
Start small enough that failure is affordable. Design well enough that success is expandable.
That's how medical AI solutions move from pilot theatre to useful infrastructure.
Turning AI Potential into Actionable Strategy
Medical AI solutions are most valuable when leaders stop treating them as a category and start treating them as a sequence of decisions. Pick the right workflow. Validate it in context. Govern it like any other clinical risk-bearing system. Then expand.
Healthcare organisations should start by selecting one pilot with a clear owner and measurable operational value. Startups should focus on solving stubborn workflow or access problems, especially where the market still under-serves vulnerable settings. That's a major opportunity because only 12% of under-resourced clinics have implemented AI due to funding and IT infrastructure constraints, as noted in this discussion of AI access gaps in underserved communities.
If your organisation is assessing where medical AI fits, Cleffex Digital Ltd can support the practical side of the journey, from secure software design and workflow integration to custom AI implementation for Canadian healthcare and life sciences environments.







