



The opportunity in Canadian health tech is large, but the margin for error is small. The Canadian healthcare SaaS market is projected to grow at a 19.53% CAGR from 2023 to 2033, according to Spherical Insights on Canadian healthcare SaaS. That number matters less as a market headline than as a product signal. Clinics, provider groups, and healthcare startups are actively looking for software that removes admin friction, supports remote care, and doesn't create new privacy risk.
That's why healthcare SaaS product development can't be treated like ordinary B2B software. You're not just shipping features. You're fitting into regulated workflows, handling sensitive patient data, and asking busy clinical teams to trust your product during stressful work. If your onboarding is clumsy, your permissions are vague, or your integration approach is naïve, adoption stalls fast.
Teams that want a grounded view of architecture and delivery can compare approaches like Bridge Global for compliant healthcare software alongside practical guidance on healthcare software development in Canada. The useful lens is simple. Build for the clinic you serve, not the idealised enterprise workflow in a slide deck.
Introduction
Most founders enter healthcare because the problem is meaningful. Better scheduling, safer handoffs, cleaner billing, faster intake, stronger patient communication. All of that is worth building. But in healthcare SaaS product development, good intent won't save a weak product strategy.
A first build usually fails in one of three places. The team picks a problem that isn't painful enough. It designs for administrators and forgets clinicians. Or it treats compliance as paperwork to handle after launch. In Canada, that last mistake is especially expensive because privacy, consent, storage, and data-sharing decisions shape the product from the first architecture sketch.
The practical path is narrower, but it works. Start with workflow truth. Scope a small product that solves one operational problem well. Build security and interoperability into the foundation. Then validate the product in the messy reality of a clinic, not in a clean demo environment.
Laying the Foundation: Discovery Requirements and Clinical Workflows
Canadian Medical Association reporting on administrative burden has made one pattern hard to ignore. Clinicians lose meaningful time to paperwork, fragmented systems, and repeated data entry. In healthcare SaaS product development, weak discovery adds to that burden fast. It produces software that looks reasonable in a backlog review and breaks down in a live clinic.
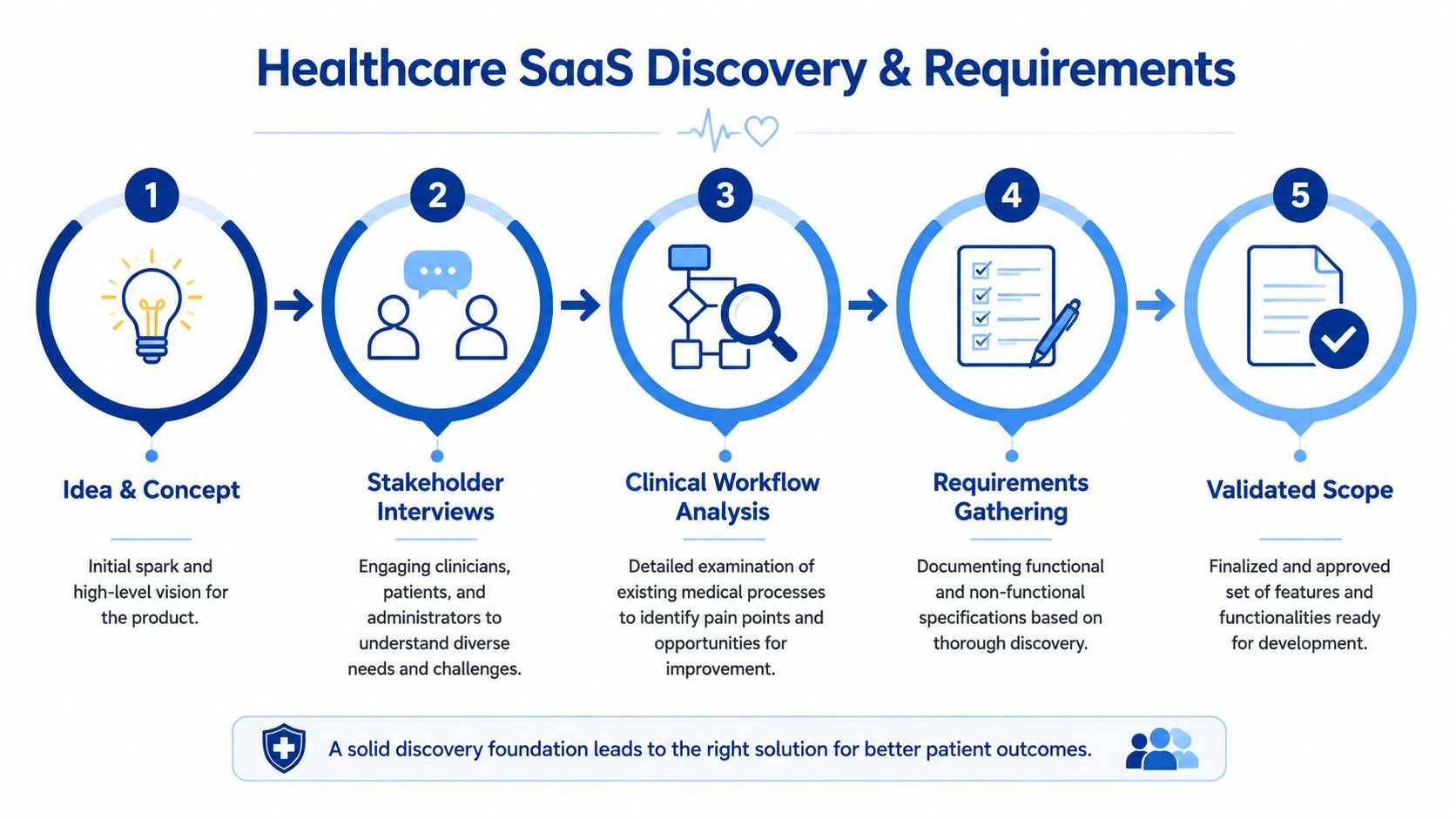
Start with workflow, not features
Small clinics do not buy software as a feature list. They experience it through bottlenecks. A receptionist is checking insurance details while answering the phone. A physician is trying to finish charting between visits. A practice manager is reconciling billing exceptions as the day concludes. If your team has not watched that work happen, the requirements are still guesses.
Map the current state before you scope the MVP. Use shadowing, screen-share walk-throughs, and document review. Follow one patient journey from booking or referral through intake, care delivery, billing, and follow-up. Capture where staff re-enter information, where they leave the EMR to finish a task, and where delays create downstream risk.
A team that cannot draw the current workflow from first contact to closed-loop follow-up is not ready to write user stories.
Stakeholder mapping in Canada is more complicated than it looks
Early teams often interview one physician champion and one technical contact, then call discovery complete. That misses how smaller Canadian organisations operate. In a family health clinic or allied care practice, the privacy officer may be external, the IT support may be part-time, the clinic manager may control budget, and the front desk may decide whether the product survives week two.
A useful stakeholder map includes five groups:
Clinical users who need speed, context, and safe defaults.
Administrative staff who need fewer manual handoffs and fewer exceptions.
Clinic leadership who need pilot success to translate into a workable business case.
Privacy or compliance owners who need clear answers on collection, disclosure, access, and retention.
Integration counterparts from EMRs, billing systems, labs, or messaging vendors.
Conflicts show up early. A clinician may want one-click access from anywhere. A privacy lead may require stronger role checks, session controls, or tighter visibility by location. Product teams have to choose deliberately and document why.
Define the smallest useful product
Healthcare MVPs fail when they try to solve an entire operating model in one release. The better move is narrower scope with clearer proof of value.
Good first products usually target one painful workflow. Referral intake. Consent capture. Patient messaging for a specific use case. Internal task coordination around follow-up. Scheduling rules for multi-provider clinics. Those are easier to test, easier to explain to a buyer, and easier to assess for PHIPA and PIPEDA impact.
Use a simple screen for scope:
| Product question | Good signal | Risk signal |
|---|---|---|
| Is the pain obvious in daily operations? | Staff already use spreadsheets, sticky notes, inbox workarounds, or duplicate entry | The problem sounds strategic but rarely blocks the day |
| Is there a clear buyer and internal owner? | One person can approve a pilot and assign staff time | Budget, authority, and accountability sit with different people |
| Can the clinic judge value in weeks, not quarters? | Time saved, fewer errors, or faster turnaround is visible quickly | Success depends on several teams changing behaviour at once |
| Is the compliance scope clear enough to design for now? | Data flows, roles, and disclosures are known | Data sharing assumptions are vague or still changing |
That discipline matters more in Canada than many first-time founders expect. Provincial privacy obligations, custody questions, and local hosting expectations can change product scope before design starts. Teams that need a grounded delivery perspective often review what to look for in a healthcare technology partner in Canada before they commit to discovery outputs and pilot planning.
Clinical workflow discovery has to include interoperability reality
Interoperability decisions belong in discovery, not after the UI is approved. Many startup teams assume integration will be a later technical task. In clinics, it changes product value from day one.
The practical challenge is whether your product can communicate with older EMRs, billing tools, scheduling platforms, and provincial workflows without creating more work for staff. Some clinics can support modern APIs. Others still depend on exports, secure file exchange, or vendor-mediated integrations. That is a product constraint, not an engineering footnote.
For CRM and patient engagement teams comparing healthcare-specific data models, MarTech Do on Health Cloud gives a useful view of how platform structure affects care coordination use cases. It also highlights a trade-off new teams often miss. Rich patient relationship models are attractive, but they add implementation weight that small clinics may not be able to absorb early.
Privacy by design needs requirements, not slogans
In Canadian healthcare, privacy by design starts as a requirements exercise. If your product handles personal health information, discovery has to answer practical questions before design begins.
Document these items clearly:
What personal health information enters the system
Which users need access, and for what exact purpose
Whether the clinic is acting as a custodian, agent, or service provider in the workflow
Where data is stored, processed, backed up, and supported
What disclosures, consents, and notices the clinic needs
What events require audit logs
What data the product should never collect in the first place
Many early builds drift off course. Teams write broad requirements such as "must be PHIPA compliant" and move on. That does not help design intake forms, role permissions, support access rules, record retention settings, or cross-border vendor reviews.
Discovery should end with artefacts that product, engineering, compliance, and clinic leadership can all use. Current-state workflows. Future-state workflows. A role matrix. A data flow map. A system inventory. A short list of assumptions that still need validation. If those documents are weak, the build will be expensive to correct later.
Building a Compliant Core Architecture and Security by Design
A single weak architectural decision can create years of compliance debt in healthcare SaaS. In Canadian clinic settings, that debt usually shows up in three places first: access control gaps, incomplete auditability, and data flows that no one mapped clearly enough before launch.
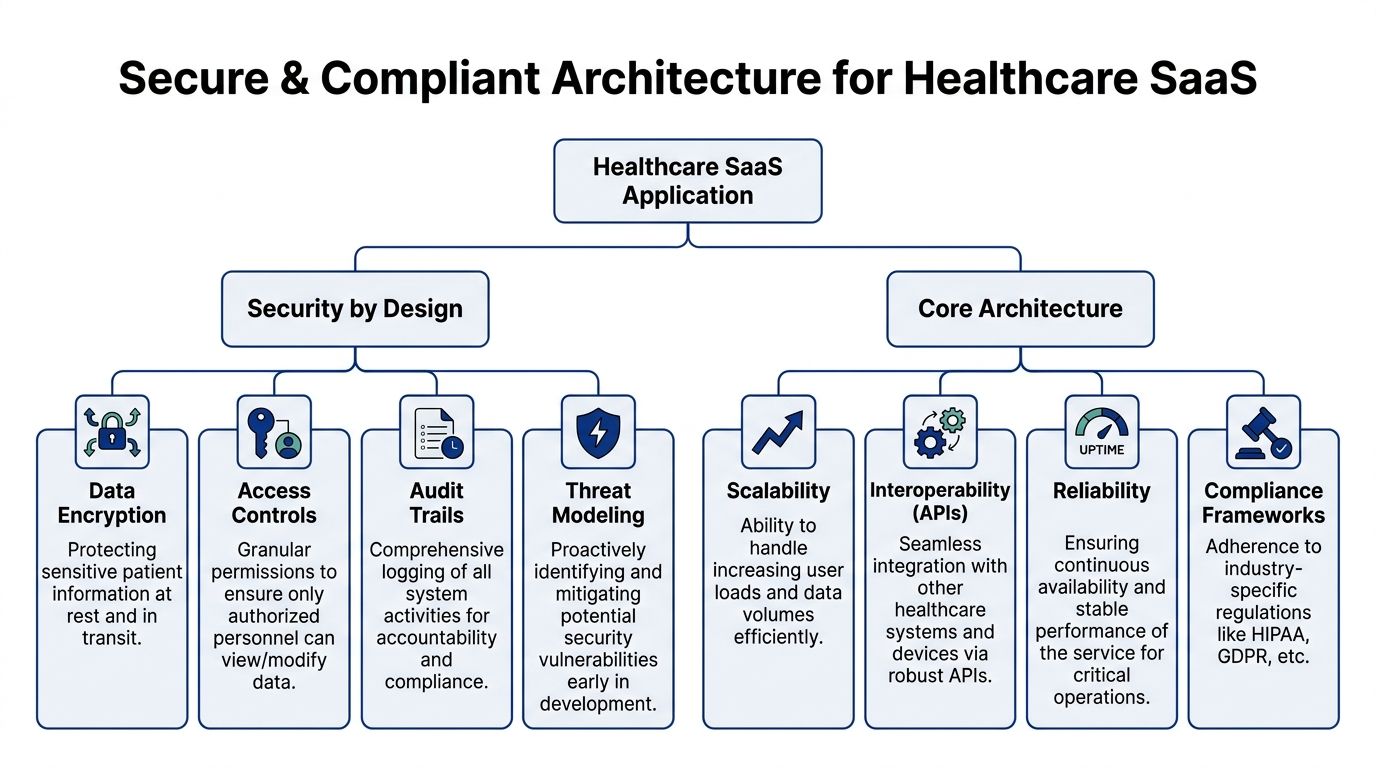
Privacy by design has to show up in system behaviour
For small clinics and startups in Canada, privacy by design is less about policy language and more about how the product behaves under PHIPA, PIPEDA, and day-to-day operational pressure. A clinic should not need heroic internal discipline to keep patient data handled properly. The application should make the safer path the default one.
That means architectural choices such as scoped access tokens, tenant isolation, field-level permissions for sensitive data, support tooling that masks personal health information, and audit events that are useful in an actual investigation. If a physician can see one record too many, or a support agent can impersonate users without a clear log trail, the problem is not training. The system was set up badly.
I advise teams to design for minimum necessary access from the first sprint.
Collect only the data tied to a defined clinical or operational use case
Separate identity data from encounter or workflow data where the product can support it
Restrict production access for engineers and support staff
Log record access, exports, consent changes, permission changes, and administrative overrides
Set retention and deletion rules in code, not in a policy document no one follows
These decisions are harder to retrofit than founders expect. Once clinics have live data, every schema change, retention update, and permission redesign gets slower, riskier, and more political.
Choose an architecture your team can actually run
Early teams often reach for microservices because they expect future scale. In healthcare, scale is only one variable. Security review, auditability, deployment discipline, and incident response matter just as much.
A modular monolith is usually the better starting point for a product serving independent clinics with one or two core workflows. It is easier to reason about, easier to secure consistently, and easier to validate when you need clear evidence of who can access what. Microservices start to make sense when domains are separate, integration volume is rising, and the team has enough engineering maturity to handle service-to-service auth, centralised logging, secrets management, and distributed tracing without cutting corners.
| Option | Best fit | Main trade-off |
|---|---|---|
| Modular monolith | Early-stage products with scheduling, intake, charting, or billing in one bounded product | Strong discipline is needed to keep module boundaries clean |
| Microservices | Broader platforms with distinct domains, external APIs, or uneven scaling patterns | More infrastructure, more failure points, more security configuration to maintain |
I have seen small HealthTech teams lose months building service boundaries they did not need yet. I have also seen teams keep everything in one codebase too long and pay for it later in release bottlenecks. The right answer depends on product scope, team maturity, and how many regulated workflows sit inside the platform.
Security controls should be explicit, testable, and boring
Healthcare security should not rely on good intentions. It should rely on controls you can configure, test, and prove. The OWASP Cryptographic Storage Cheat Sheet is a better baseline for encryption decisions than generic healthcare trend articles because it gets specific about key management, algorithm selection, and storage risks.
In practical terms, the core baseline includes:
Encryption in transit and at rest for personal health information and sensitive operational data
Strong key management with separation between encrypted data and key material
Multi-factor authentication for administrators, privileged users, and remote access paths
Role-based access control aligned to clinic roles, not generic user buckets
Audit trails that are tamper-aware and easy to review during an incident
Threat modelling before major releases, especially for integrations, AI features, and patient messaging
Centralised logging, alerting, and backup validation
Canadian teams also need to make a clear decision about data residency and vendor exposure. Some clinics will accept cloud hosting outside Canada with the right contractual and risk controls. Others will not. That decision affects hosting, backups, support processes, subprocessors, and procurement friction. It should be made early.
A simple rule helps. If your system cannot answer who accessed a patient record, what changed, from where, and under which role, the product is not ready for clinical trust.
For teams evaluating broader care-platform patterns, MarTech Do on Health Cloud is a useful reference point for patient relationship workflows and data model choices, even if you are not building on Salesforce. For a more practical Canadian implementation view, this guide to healthcare compliance software development covers the constraints that shape architecture decisions for clinics and emerging HealthTech products.
The Build Phase: Clinical UX and System Integration
The build phase is where good intentions meet real constraints. In healthcare, the two constraints that humble teams fastest are clinical UX and interoperability. You can have excellent engineers and still fail here if no one on the team understands how care delivery feels in practice at the point of use.

Clinical UX is about safety and speed
Healthcare interfaces aren't judged like consumer apps. Clinicians don't want delight. They want confidence, legibility, and minimal friction.
A useful screen should support interrupted work. It should preserve context, make the next action obvious, and avoid forcing memory-based navigation. During a busy shift, every unnecessary modal, hidden control, or ambiguous label increases cognitive load.
Design teams should test for these realities:
Can a user complete a task with one hand on a tablet or touchscreen?
Are touch targets large enough for fast use in clinical settings?
Does the colour system preserve contrast under harsh lighting?
Can users distinguish alerts, warnings, and informational messages instantly?
Does the flow mirror the sequence of work in the clinic, not the database schema?
A surprisingly common mistake is building around a backend object model. Real users think in appointments, encounters, referrals, messages, and tasks. They don't think in entity relationships.
Integration work is product work
Many teams still treat interoperability as a technical stream that sits beside the product. In healthcare SaaS product development, integration is the product for a lot of customers. If your software can't exchange data reliably with existing systems, it becomes another screen staff must maintain manually.
The development lifecycle in this sector requires a dedicated team that includes developers, designers, and in-house compliance experts working against standards such as HIPAA, PIPEDA, PHIPA, HL7, and FHIR, according to SysCreations on building healthcare SaaS software. That mix matters because data exchange decisions affect compliance, UX, and delivery timelines at the same time.
What works in integration projects
The practical challenge is rarely “do we support FHIR?” The key question is whether your product can communicate with older EMRs, partial APIs, inconsistent data fields, and weak network conditions without becoming brittle.
What tends to work:
Build an integration abstraction layer
Don't scatter vendor-specific logic throughout the app. Keep adapters isolated so one partner system doesn't contaminate your product architecture.Design for asynchronous behaviour
Not every clinic operates in ideal connectivity conditions. Queue non-critical syncs, handle retries safely, and show users clear sync status.Map workflows, not just fields
A technically valid data exchange can still be operationally useless if timing, ownership, or trigger conditions don't match the clinic's process.Create fallback states
If an external system is down or slow, users need a safe next step. Read-only access, local drafts, and deferred submission are often better than hard failure.
The hardest integration projects aren't blocked by standards. They're blocked by assumptions that every partner system behaves cleanly.
Team shape matters during build
A generalist dev team without healthcare product support will miss edge cases. A pure compliance team without product instincts will over-constrain the experience. You need both.
At this stage, one delivery model that some organisations use is a specialist engineering partner such as Cleffex Digital Ltd, particularly when they need support across product engineering, compliant healthcare workflows, and scalable software delivery without building every capability internally. That only works if the partner joins workflow reviews, design critique, and release planning. Healthcare products fail when delivery is reduced to ticket execution.
From Code to Clinic Validation, Deployment, and Scalability
A feature-complete product still isn't clinic-ready. The hard part now is proving the software behaves safely in real environments, then deploying it in a way that can support growth without creating new compliance risk.
A reliable Canadian healthcare SaaS delivery method usually combines dependable cloud infrastructure, microservices where they're justified, and continuous compliance pipelines that verify controls against frameworks such as HIPAA, SOC 2, and HITRUST.
Validation has to go beyond QA
Standard QA catches bugs. It doesn't prove clinical usability, operational fit, or safe deployment.
Validation should cover at least four lenses:
| Validation type | What to test | Why it matters |
|---|---|---|
| Functional testing | Workflows, permissions, failure states | Basic product reliability |
| Usability testing | Real tasks with actual clinic users | Reveals friction and safety risks |
| Security testing | Access paths, role leaks, logging, exposure points | Protects sensitive data and trust |
| Pilot validation | Live use in a controlled environment | Exposes environmental and workflow issues |
The most useful pilots are narrow. One clinic, one workflow, one ownership group. Broad pilots often generate noise instead of insight because too many variables move at once.
Deployment decisions shape future margins
Cloud deployment is rarely just an engineering preference in healthcare. It affects security operations, tenant separation, support effort, and customer trust.
For small clinics and startups, the common deployment trade-offs look like this:
Single-tenant setups offer clearer separation and can simplify some customer conversations, but they add operational overhead.
Multi-tenant architectures usually fit the SaaS model better, but tenant isolation, permissions, configuration boundaries, and audit visibility have to be handled carefully.
Shared core with customer-specific configuration often gives the best balance if the product serves many clinics with similar workflows.
If your target buyers are independent clinics, keep implementation simple. They usually don't want a long deployment project. They want a secure, understandable rollout with minimal disruption. Hospital groups and insurers often need more governance, stronger procurement handling, and deeper reporting controls before they'll move.
Speed helps only when controls keep up
Fast shipping is useful. Reckless shipping isn't. Teams exploring ways to reduce build time often review resources like Appjet for rapid app shipping to understand where automation can remove repetitive engineering work. In healthcare, that acceleration must sit behind approval gates, test coverage, and compliance checks that are specific to the product's risk profile.
A practical deployment rhythm usually includes:
Release gates tied to security and privacy review
Environment parity so staging reflects production closely
Automated checks for access control regressions and configuration drift
Rollback paths that teams have already rehearsed
Operational dashboards for uptime, queue health, integration failure, and audit log integrity
If a release process can't explain how a permissions change was tested, it's not mature enough for patient-facing workflows.
Go-to-Market and Beyond Pricing Operations and Growth
A live product solves only half the problem. The rest is getting buyers to trust it, structuring pricing so adoption isn't blocked, and running operations tightly enough that growth doesn't erode service quality.
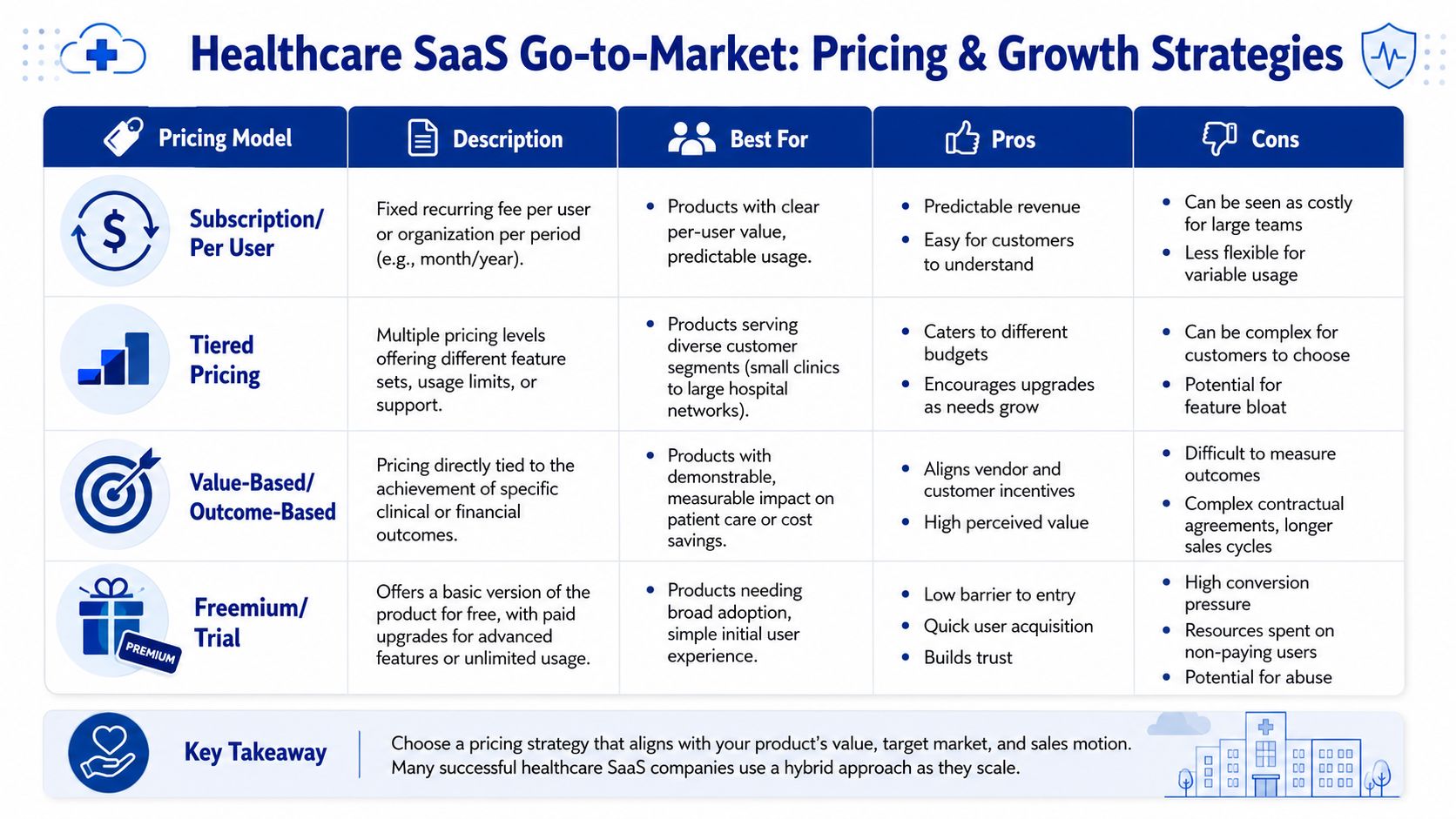
Pick pricing that matches the buyer's budgeting logic
Many teams choose pricing based on investor familiarity instead of customer behaviour. That creates friction during procurement.
A better way is to align pricing with how each customer type evaluates software:
| Customer type | Pricing model that often fits | Why |
|---|---|---|
| Small clinics | Subscription or simple tiered pricing | Easy to budget, low admin overhead |
| Multi-site provider groups | Tiered pricing with implementation scope | Supports variation in workflow and support needs |
| Payers or enterprise buyers | Contracted platform pricing or outcome-linked structures | Procurement expects negotiation and measurable business value |
| Startups embedding healthcare workflows | Usage-sensitive commercial terms | Lets them scale without heavy fixed cost too early |
For clinics, complexity kills deals. If they need three calls to understand your invoice logic, your model is too complicated.
Trust is the real go-to-market engine
Healthcare sales cycles are slower because buyers are evaluating risk, not just functionality. They want to know whether the product fits their workflow, whether your team responds well under pressure, and whether the rollout will create disruption.
What helps most:
Tight pilot scopes that answer one operational question clearly
Implementation plans that show who does what and when
Security and privacy documentation written for non-technical stakeholders
Referenceable use cases by clinic type, workflow, or operating model
Clear support commitments for incidents, access issues, and downtime
Freemium can work for simple administrative tools, but it's harder in products with compliance-heavy onboarding or integration work. Outcome-based pricing can be appealing when the product's value is measurable and attributable, but it often brings a longer contracting process. Subscription and tiered approaches remain easier for most clinic-focused products because they reduce ambiguity.
Operations decide whether growth sticks
A growing healthcare SaaS business needs disciplined post-launch operations. That means active monitoring, incident response ownership, and a roadmap process informed by real usage, not just customer requests.
Build these habits early:
Monitor what matters
Watch workflow failures, sync delays, auth issues, and permission anomalies, not just uptime.Write an incident playbook
Teams should know how to respond to security events, degraded integrations, and service outages before any of them happen.Review user feedback in context
A feature request from a physician, admin lead, and operations owner may describe the same underlying problem differently. Product teams need to reconcile that, not count votes.Protect roadmap discipline
Healthcare buyers often ask for adjacent features. Some requests are strategic. Others are custom work disguised as product demand.
The companies that last don't chase every request. They keep refining a core workflow, hardening trust, and expanding only when the operational model can support it.
Conclusion
Healthcare SaaS product development rewards discipline more than speed. Teams that succeed understand clinical workflows thoroughly, build privacy and security into the architecture, respect the realities of interoperability, and treat validation as part of product strategy rather than a final check. In Canada, that discipline matters even more because PIPEDA, PHIPA, and data handling choices affect the product from the start.
If you're building for clinics, hospitals, or health startups, keep the scope honest, the controls strong, and the workflow central. That's what gets software from a promising demo into daily clinical use.
If you're planning a healthcare SaaS product and need a team that understands secure architecture, Canadian compliance realities, and practical product delivery, Cleffex Digital Ltd can support the build from discovery through deployment with a grounded, engineering-led approach.







