



A hospital billing clerk opens what looks like a routine vendor invoice. Minutes later, accounts can't reach a shared drive, the help desk starts fielding password reset calls, and clinical staff begin asking why records are loading slowly. That's how data security failures usually begin. Not with drama, but with one ordinary action inside a busy system.
The High Stakes of Patient Data Protection
The clearest Canadian example is LifeLabs. In 2019, a cyber-attack on the Toronto-based testing company compromised the electronic health records of approximately 15 million patients, exposing names, addresses, health card numbers, and lab results, as reviewed in The Lancet's analysis of the LifeLabs breach and its policy impact30030-3/fulltext). For any hospital IT director, that's the practical meaning of data security in healthcare information systems. A breach doesn't stay in the server room. It reaches registration desks, call centres, clinicians, privacy officers, executives, and patients.
What made that event so consequential wasn't just the scale. It exposed how fragile healthcare operations become when sensitive data sits inside complex digital environments with too much trust, too little segmentation, and weak assumptions about who can access what. In healthcare, confidentiality matters, but so do availability and integrity. If staff can't trust the system or can't reach it, care suffers.
What hospital leaders often underestimate
Most organisations still start from the wrong question. They ask, “Are we compliant?” before they ask, “How does an attack move through our people, systems, and vendors?” Compliance is necessary. It isn't a defence strategy.
A stronger approach treats security as a layered operating model:
Technical controls such as encryption, MFA, secure DNS, and monitored access logs
Operational discipline such as incident response, access reviews, and vendor governance
Human judgement from staff who know what suspicious behaviour looks like in their specific role
Practical rule: If your staff can access patient data, they are part of your security perimeter, whether they work in IT, billing, records, HR, or procurement.
That's why the strongest programmes combine infrastructure hardening with role-specific staff behaviour. If you want a patient-facing companion resource to share internally or adapt for awareness campaigns, this roundup of critical patient data security advice is useful because it translates security concerns into concrete handling practices.
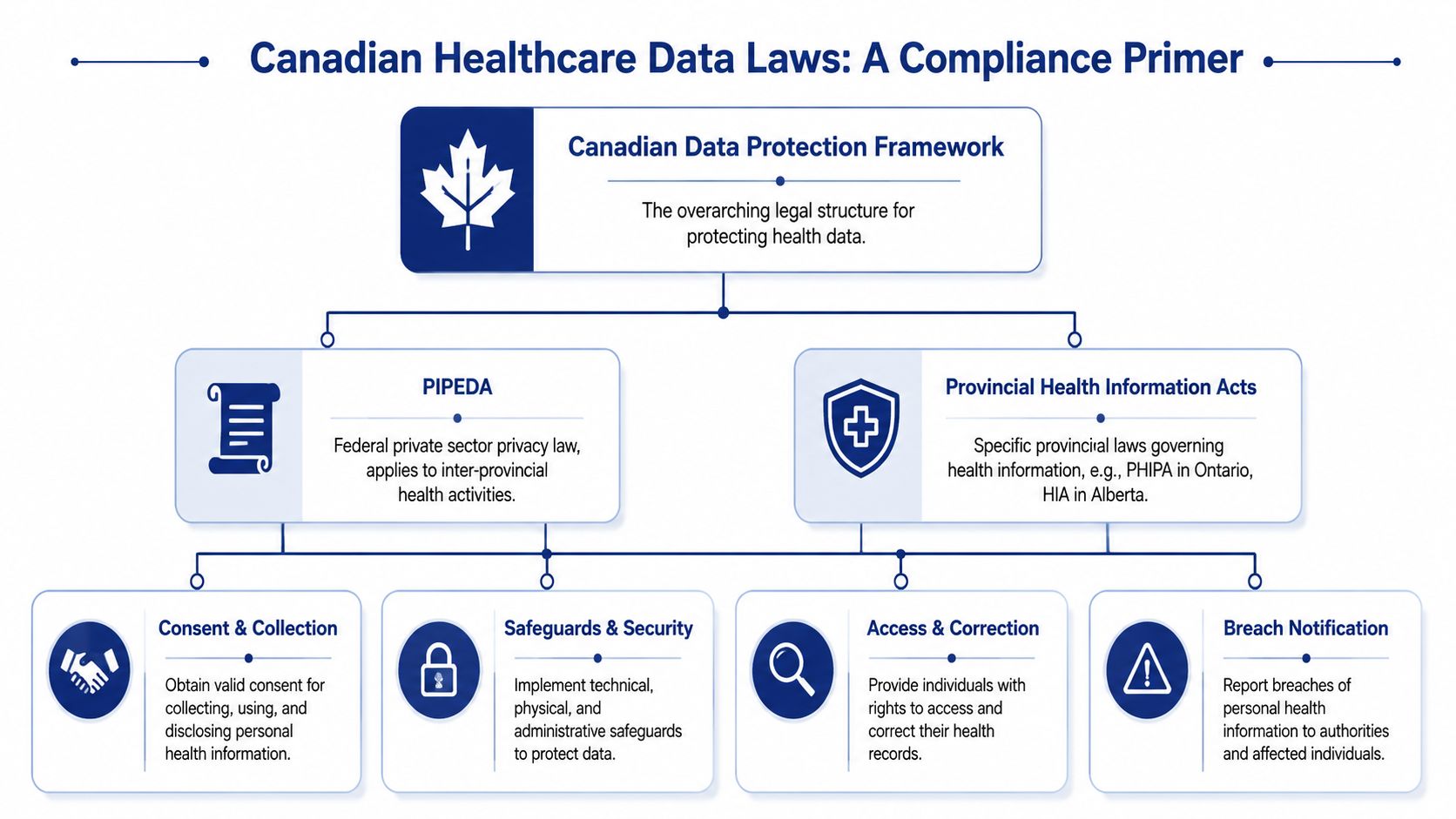
Your Core Responsibilities Under Canadian Law
Canadian healthcare organisations don't get to treat privacy and security as separate projects. The legal baseline already expects both. At the federal level, PIPEDA creates mandatory breach reporting and notification obligations, and national policy direction also points organisations toward stronger safeguards such as encryption by default and Canadian data residency, as outlined in the Canada health data governance country report.
What that means in practice
An IT director usually needs to translate legal duties into operating controls. The most important ones are straightforward:
Protect personal health information with real safeguards: That includes administrative, technical, and physical measures, not just policy language.
Report breaches when required: If an incident meets the threshold, your organisation must notify affected individuals and the appropriate authority.
Control where data lives and who can reach it: Residency, hosting, and access design affect both enforcement and risk.
Support access and correction rights: Systems must let authorised staff handle legitimate record requests without bypassing security.
Security safeguards under Canadian law are not satisfied by having a policy manual on a shared drive. They have to show up in system design, identity controls, monitoring, and response procedures.
Federal law is the floor, not the ceiling
Provincial health information laws add more specificity, especially around custodianship, permitted disclosure, and operational handling. Alberta's Health Information Act is a good example of how provincial requirements can sharpen expectations around health data governance. For delivery teams building or modernising regulated platforms, this guide to healthcare compliance software development is worth reading because it frames compliance as an engineering requirement rather than a legal afterthought.
A practical way to manage the legal environment is to maintain one control matrix that maps each obligation to:
| Legal duty | Operational owner | Evidence you should keep |
|---|---|---|
| Breach notification | Privacy officer and security lead | Incident logs, decision records, notification workflow |
| Safeguards | IT and platform owners | MFA settings, encryption configuration, audit trails |
| Access and correction | HIM and application owners | Request handling process, approval records |
| Data handling and residency | IT architecture and procurement | Hosting contracts, vendor reviews, data flow maps |
Where organisations often fail
The common failure isn't ignorance of PIPEDA. It's fragmentation. Privacy owns policy, IT owns infrastructure, procurement signs cloud contracts, and nobody owns the full data path. In hospitals, that usually leads to inconsistent controls between core clinical systems, departmental applications, backup environments, and third-party platforms.
That's avoidable if one team is accountable for end-to-end governance of healthcare data, not just endpoint security or legal paperwork.
Common Threats and Digital Attack Vectors
Think of a hospital as a fortress with too many side doors. The main gate might be guarded, but attackers rarely start there. They look for the loading dock, the unsecured service entrance, or the staff member who holds the wrong key.
In healthcare, the biggest problem is still compromised systems. Compromised IT systems account for up to 80% of healthcare data breach incidents, which is why access monitoring and formal incident response can't be optional, according to this healthcare data security overview citing OCR patterns and incident response practice.
The attack paths that matter most
A few patterns show up repeatedly in real environments.
Phishing through routine workflows: A fake invoice lands with Accounts Payable. A password reset message reaches the help desk. A benefits attachment goes to HR. The email doesn't need to fool everyone. It only needs one person with enough access.
Ransomware through flat networks: An attacker gets into one workstation, finds broad internal trust, and then moves laterally into shared systems, storage, or identity infrastructure.
Insider misuse or error: Staff export data for convenience, forward records to personal email, leave portable devices unsecured, or browse files outside their role.
Vendor-linked exposure: A trusted integration, support account, or cloud administration path becomes the quiet entry point.
What these threats look like inside a hospital
The threat isn't abstract. It usually arrives dressed as normal work.
| Attack vector | Typical healthcare scenario | Why it succeeds |
|---|---|---|
| Phishing | Finance receives a “past due” vendor message | Staff are busy and the message matches workflow |
| Credential theft | IT admin reuses a password or approves a fake prompt | Privileged users are highly targeted |
| Ransomware | Malware spreads from one endpoint to shared systems | Networks are insufficiently segmented |
| Insider error | Clerk downloads more records than needed | Access rights are broader than duties |
The organisations that catch these incidents early usually have two things in place. Log review that someone actually performs, and a response process that people have rehearsed before the crisis.
What doesn't work
Annual awareness slides don't stop a live phishing attempt. Neither does a beautifully written policy nobody uses. Hospitals also lose time when they treat every suspicious event as an IT ticket instead of a possible security incident.
What works is tighter recognition of abnormal behaviour. That includes impossible logins, unusual file access, repeated MFA prompts, unexpected exports, and admin actions performed outside normal maintenance windows. The earlier your team spots those signals, the smaller the blast radius.
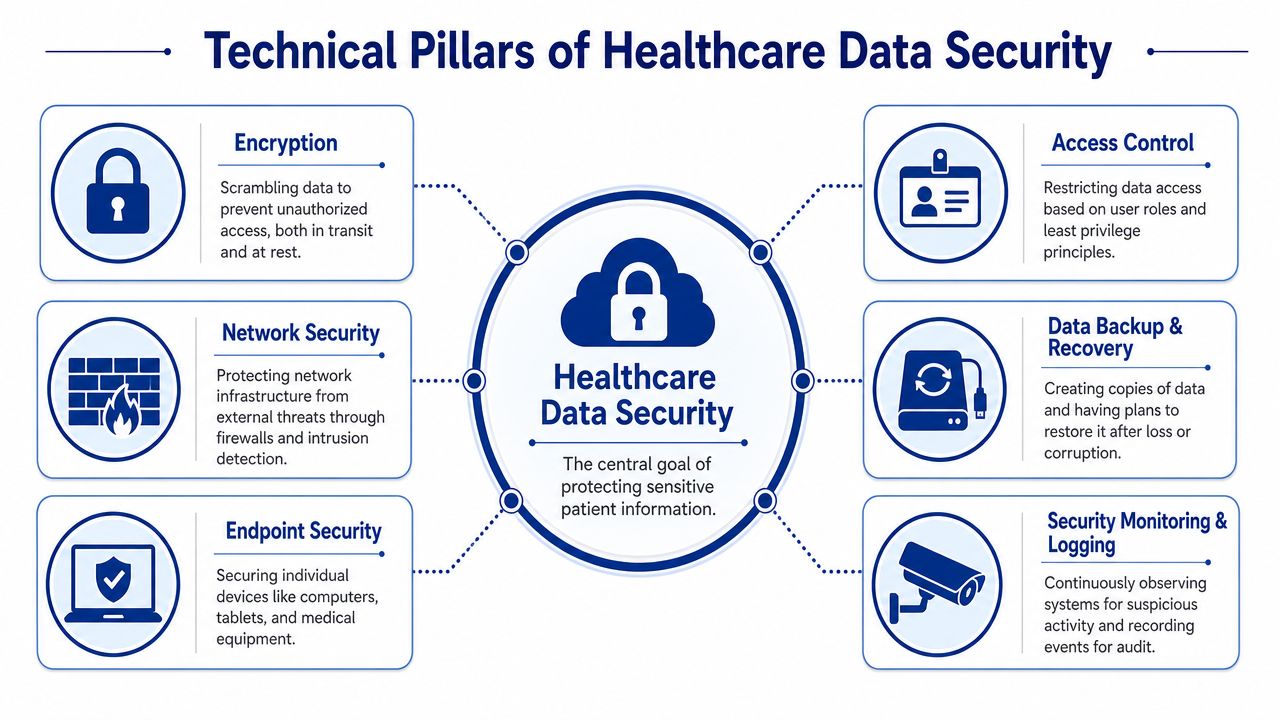
Building Your Technical Defence Systems
Most hospital environments don't fail because they lack tools. They fail because controls are unevenly deployed, poorly integrated, or never tuned to healthcare workflows. Good technical defence is layered, boring, and consistent.
One of the most important Canadian design choices is encryption by default. Health data should be converted into key-encrypted formats before storage, and that's often paired with data residency on Canadian soil to strengthen the enforcement power of Canadian authorities, as discussed in this peer-reviewed analysis of encryption, localisation, and sovereign cloud strategy.
Start with the controls that change outcomes
If I'm advising a hospital, I prioritise the controls that reduce both likelihood and impact.
Encrypt data before you store it
Encryption at rest matters, but design-by-default encryption matters more because it assumes interception is possible. If an attacker or unauthorised party reaches the data stream or underlying storage, the information should still be unusable without the right key management.
The trade-off is operational. Encryption affects integrations, key rotation, application performance testing, and support workflows. But in healthcare, that complexity is worth carrying.
Tighten identity and access management
Most breaches don't require a genius attacker. They require an account with too much reach.
Use these IAM rules:
Enforce MFA everywhere feasible: Privileged accounts first, remote access second, then all standard users.
Apply least privilege by role: Billing staff don't need broad clinical data access. Temporary staff shouldn't inherit permanent rights.
Review accounts on a schedule: Dormant accounts, shared credentials, and stale vendor access create silent risk.
Separate administrator identities: Staff shouldn't use the same account for email, routine work, and admin actions.
For teams building or reworking digital health products, this guide to building secure healthtech applications is practical because it ties access design, encryption, and application architecture together.
Protect the network and the endpoints
A flat network is an attacker's gift. Segment clinical systems, administrative systems, and high-trust infrastructure. Restrict east-west movement wherever you can. Firewalls, VPNs, and secure Wi-Fi design are still basic requirements, not optional extras.
Protected DNS also deserves more attention. Services such as Canadian Shield can help block known malicious destinations before users ever reach them. That won't solve a compromised credential problem, but it can cut off one common path for phishing follow-through and malware download.
Monitor like you expect abuse
Logging is only useful if someone can answer three questions fast:
Who accessed the data
What they did
Whether that behaviour fits the role
Your logs should cover identity events, administrative actions, privileged access, large exports, failed login clusters, and configuration changes. The goal isn't to collect everything forever. The goal is to detect what matters early enough to contain it.
Operational test: If your SOC or IT team sees a suspicious export from a non-clinical account at 2 a.m., can they identify the user, isolate the session, and confirm data scope quickly? If not, your monitoring stack is incomplete, even if your dashboard looks impressive.
Strengthening Your Human Firewall Through Training
Healthcare security programmes often invest heavily in infrastructure and then underinvest in behaviour. That's a mistake. The human layer is where many incidents begin, especially in hospitals where dozens of non-clinical roles touch patient information every day.
The blind spot is now too obvious to ignore. A 2025 HIMSS study found that 72% of breaches stem from employees with EHR access but no clinical duty, while 47% of Canadian healthcare organisations admit their training is generic and not role-specific, according to this discussion of the healthcare human infrastructure gap in Canada. That should change how every hospital trains staff.
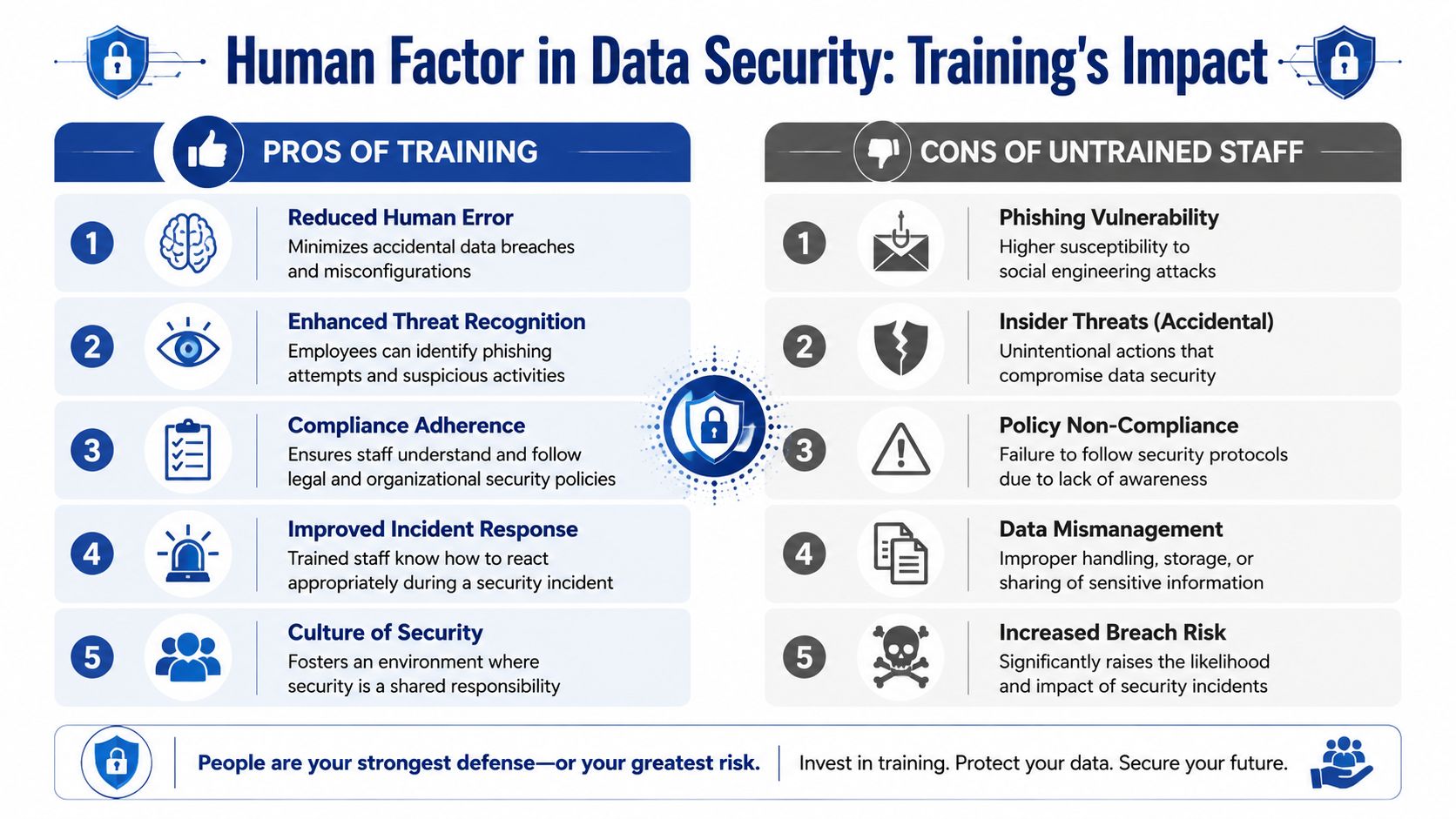
Generic annual training doesn't match real risk
A billing clerk, an HR coordinator, a records analyst, and a domain administrator don't face the same threats. Yet many organisations give them the same slide deck once a year and call it awareness. That format may satisfy a checklist. It won't change behaviour during a live incident.
Role-based training works better because it maps security decisions to actual tasks.
| Role | What they need to recognise | What they need to do |
|---|---|---|
| Billing and finance | Fake invoices, payment diversion, unusual attachments | Verify requests out of band, report suspicious messages |
| HR and administration | Payroll phishing, employee record mishandling | Limit disclosure, follow secure document handling |
| Health records staff | Improper access requests, over-disclosure | Validate request authority, log exceptions carefully |
| IT admins | Privilege abuse, MFA fatigue attacks, risky changes | Use separate admin accounts, document and review changes |
Build training around decisions, not slogans
Good training is short, repeated, and tied to workflow. Staff don't need abstract lectures on cybercrime trends. They need to know what to do when:
An email requests urgent payment changes
A physician asks for access outside the usual process
A vendor wants temporary remote support
A manager requests a spreadsheet export “just for today”
A laptop, tablet, or phone goes missing
The strongest programmes I've seen use short scenario drills with local examples. They also involve managers, because staff copy what supervisors reward. If speed is always rewarded and verification is treated as friction, people will bypass controls.
Train staff on the point of decision. If the lesson can't be applied during a real task in under a minute, it probably won't hold during pressure.
What a credible human firewall programme includes
This doesn't require theatre. It requires discipline.
Role-specific modules for non-clinical and privileged users
Clear reporting paths so staff know where suspicious activity goes
Manager reinforcement in finance, HR, records, and IT
Access reviews that remove rights no longer needed
Portable device rules that reflect actual patient-care need
Incident rehearsals so teams know their first move, not just the policy name
Measure behaviour, not attendance
Completion rates are easy to collect and nearly useless on their own. Instead, look for practical signals. Are staff reporting suspicious messages? Are managers escalating unusual access requests? Are departments reducing shared accounts and informal workarounds?
The test of a human firewall is simple. When something looks wrong, do your people slow down, verify, and escalate? If they do, your programme is working. If they click first and ask later, the hospital still has a people problem.
A Scalable Security Roadmap for Your Organisation
Most healthcare organisations can't replace every legacy system, retrain every team, and rebuild every workflow at once. They need a sequence. The right roadmap is phased, measurable, and realistic enough to survive budget pressure.
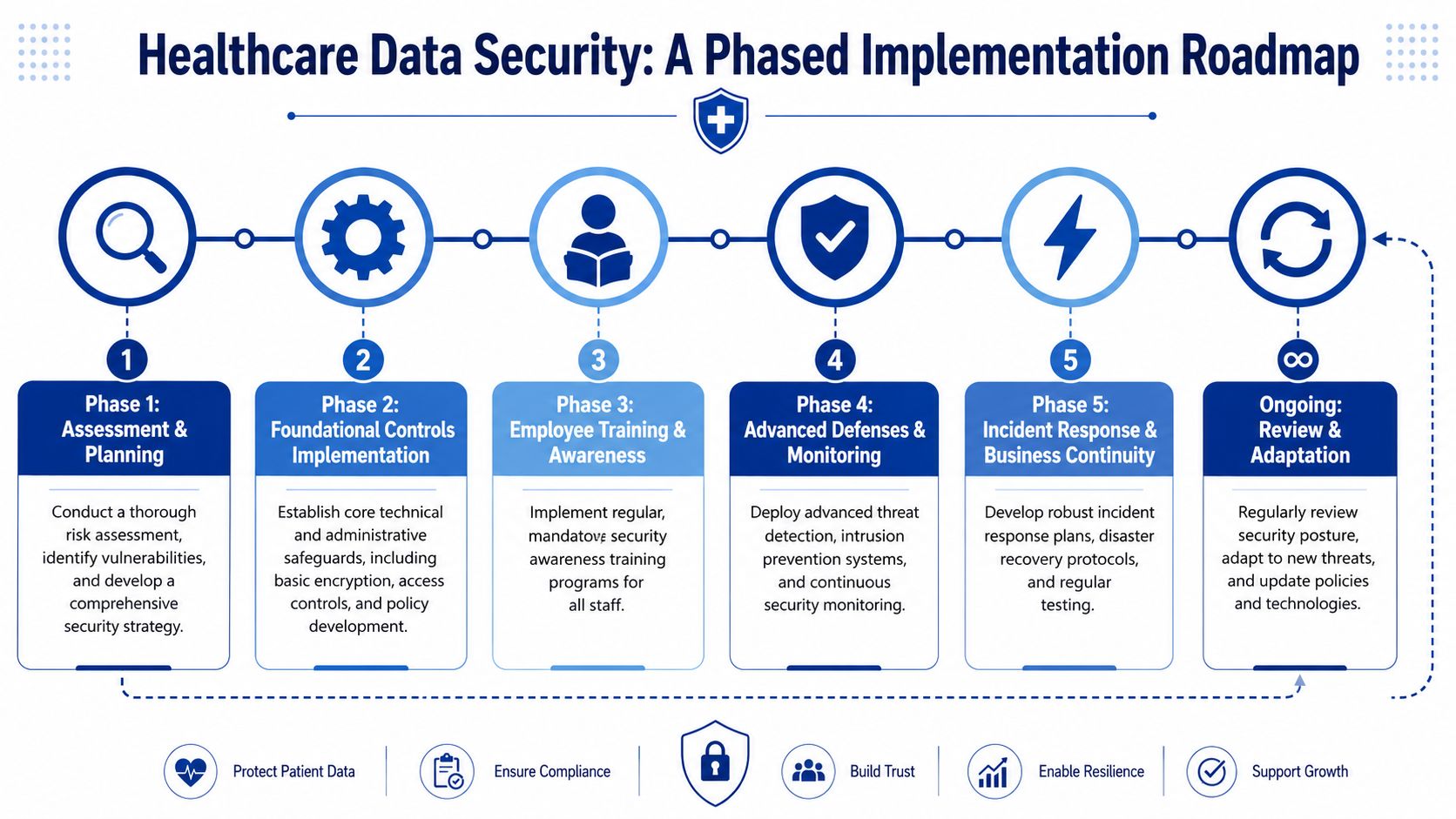
Foundational stage
Start by reducing obvious exposure.
Map your sensitive data so you know where patient information is stored, processed, exported, and backed up
Clean up access by removing shared accounts, dormant users, and unnecessary privileges
Set minimum operating rules for portable devices, remote access, and email handling
Launch role-based training for finance, HR, records, and IT first
Small clinics can get meaningful risk reduction here without a major platform overhaul.
Intermediate stage
Discipline becomes architecture.
Introduce MFA widely, formalise vendor reviews, centralise logging, and define your incident response workflow around the six phases used in common practice: preparation, identification, containment, eradication, recovery, and lessons learned. At this stage, many organisations also benefit from staff development. If your internal security lead is building capability or preparing for certification, a solid way to prepare for your CISSP exam can support stronger governance and communication with leadership.
Mature security programmes don't jump straight to advanced tooling. They stabilise access, visibility, and response first.
Advanced stage
Larger hospitals and multi-site networks should push into deeper controls:
| Stage | Priority actions | Typical outcome |
|---|---|---|
| Foundational | Access cleanup, baseline policies, targeted training | Fewer preventable errors and obvious exposures |
| Intermediate | MFA, central logging, vendor governance, rehearsed response | Faster detection and cleaner containment |
| Advanced | Segmentation maturity, stronger analytics, privacy-aware innovation controls | Better resilience across complex environments |
Advanced doesn't mean flashy. It means your organisation can absorb an incident without losing operational control. That includes tested recovery plans, stronger monitoring logic, disciplined vendor access, and governance for newer use cases such as AI-assisted workflows.
Managing Your Supply Chain and Third-Party Risk
Hospitals rarely operate on systems they built alone. EHR vendors, claims processors, cloud hosts, transcription providers, imaging platforms, and support contractors all touch the environment. If one of them has weak access controls or vague breach obligations, your hospital inherits that risk.
A practical vendor review starts before procurement, not after contract signature. Teams that need a structured process can borrow ideas from this software vendor onboarding roadmap, especially around evaluation gates and operational accountability.
Questions worth asking before you buy
Don't ask vendors if they “take security seriously”. Ask questions that force specifics:
Where is our data hosted and what subcontractors can access it
How is privileged access controlled for support engineers and administrators
What logging is available to the customer for access, exports, and admin actions
How are incidents reported and how quickly will your team be informed
What happens at contract exit when data must be returned, deleted, or migrated
Red flags in contracts and operations
Watch for vague security language, undefined breach notification terms, broad vendor rights to use service data, or support access that isn't time-bound and auditable. Also watch for platforms that make customer-side monitoring difficult. If you can't see who did what, you can't govern the risk properly.
Vendor risk management works best when procurement, IT, legal, privacy, and system owners all review the same data flow and the same support model before approval.
Third-party risk isn't separate from data security in healthcare information systems. It is part of the same control surface.
Frequently Asked Questions About Healthcare Data Security
Is cloud storage safe for Canadian patient data?
It can be, but only if the design is disciplined. Focus on encryption, access control, logging, residency requirements, and contractual limits on vendor and subcontractor access. Cloud can improve resilience, but poor configuration can also expand exposure quickly.
How can we use AI without compromising patient privacy?
Start with minimum necessary data, strong role-based access, clear auditability, and approval controls for model inputs and outputs. Don't let convenience override data handling rules. Privacy review should happen before pilots reach production workflows.
Why is secure interoperability so difficult?
Because healthcare systems were often procured at different times for different departments with inconsistent identity, data, and logging standards. The technical challenge is integration. The governance challenge is controlling access across those integrations without creating unsafe shortcuts.
What should a hospital rehearse before an incident happens?
At minimum, rehearse account compromise, suspicious data export, ransomware containment, vendor escalation, and downtime communications. Teams should know who declares the incident, who can isolate systems, who assesses privacy impact, and who communicates with leadership.
If your organisation is modernising clinical software, patient portals, integrations, or internal platforms, Cleffex Digital Ltd can help you design and build secure healthcare solutions with compliance, scalability, and practical delivery in mind.







