



Healthcare data breaches affected far more people in 2024, even though the number of large reported breaches dipped slightly. The number of affected individuals surged by 58%, and the Change Healthcare breach alone impacted approximately 192.7 million people (HIPAA Journal healthcare breach statistics).
That's the right place to start, because healthcare data security isn't an IT side project. It sits directly inside patient care, clinical operations, legal exposure, and public trust. When a clinic loses control of records, it doesn't just lose files. Staff lose confidence in their systems, patients hesitate to share information, and care delivery gets slower and riskier.
Most directors already know the basics. Use strong passwords. Patch systems. Train staff. Those matters, but they're no longer enough on their own. The harder problems now sit in places many organisations still underestimate: staff pasting patient details into public AI tools, data stored in cloud environments outside Canadian jurisdiction, old devices leaving the office without proper sanitisation, and vendors that say “secure” without answering specific questions.
Practical healthcare data security means controlling four things consistently: who can access data, where data lives, how data moves, and what happens when something goes wrong. If one of those is weak, the rest of the programme usually isn't as solid as leadership thinks.
Protecting More Than Data: Protecting Patients
Healthcare data security starts with a simple reality. Patients hand over information they wouldn't share with almost anyone else. They do that because they trust the clinic, hospital, lab, or insurer to treat that information with the same care used in treatment itself.
That trust is fragile. A system outage can delay appointments. A compromised chart can create clinical confusion. A leaked diagnosis or lab result can cause personal harm long after the technical incident is over.
What clinic leaders need to protect
A good security programme doesn't focus only on “the network”. It protects the full care environment:
Patient records: Clinical notes, lab results, intake forms, referral details, imaging, and follow-up communications.
Operational systems: Scheduling, billing, practice management software, e-prescribing tools, and integrations.
Physical assets: Laptops, phones, removable media, printers, retired servers, and old workstations.
Staff workflows: Reception, nursing, physician documentation, remote access, messaging, and file sharing.
One area that's often overlooked is asset disposal. If your clinic is replacing laptops, drives, or old servers, secure disposal has to be part of healthcare data security, not an afterthought. A practical reference for that process is the Beyond Surplus HIPAA ITAD guide, which outlines what compliant IT asset disposition should cover when devices may still contain sensitive information.
Practical rule: If a device ever stored patient data, treat retirement as a security event, not an office clean-up task.
What works and what usually fails
What works is boring, consistent control. Named owners. Defined access. Approved tools. Logged activity. Tested backups. Clear vendor terms.
What fails is informal trust: shared accounts, “temporary” exceptions that become permanent, staff using consumer tools because they're faster, and cloud decisions made by convenience rather than jurisdiction.
For a clinic director, the key shift is this: don't ask whether your organisation is “secure”. Ask whether your teams can prove where patient data is, who touched it, and how you'd respond if access was abused. That's the operational core of healthcare data security.
The Modern Threat Landscape and Its Hidden Dangers
Most healthcare organisations still frame cyber risk around phishing emails, ransomware, and stolen passwords. Those remain real threats. But the current risk picture is broader, messier, and often self-inflicted through normal daily workflow.
A useful way to look at it is to separate obvious threats from hidden ones.
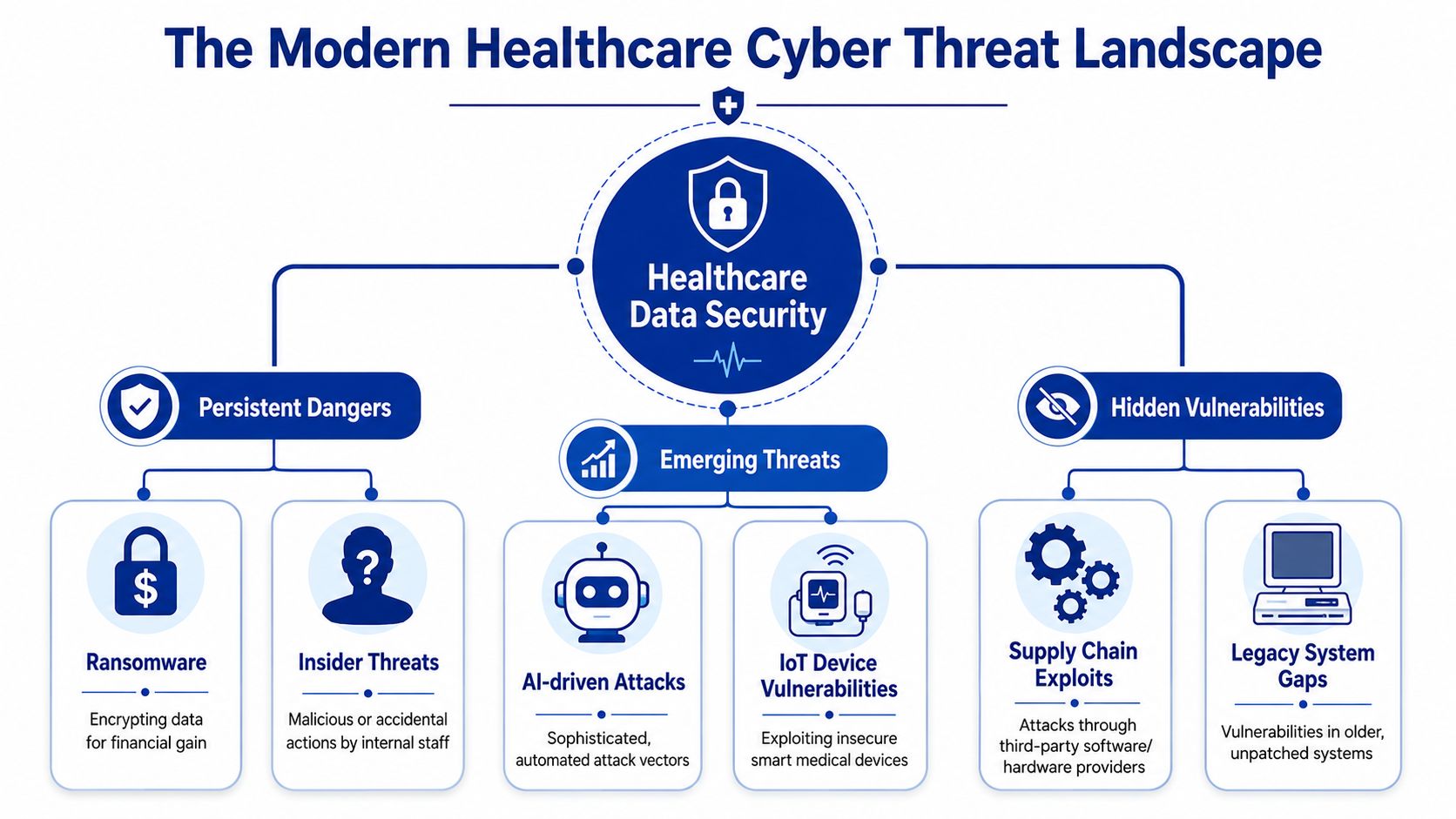
The threats leaders already recognise
Ransomware still matters because healthcare operations are time-sensitive. Attackers know reception teams need scheduling back, nurses need access to notes, and clinicians can't tolerate long downtime. That pressure changes the economics of an attack.
Insider risk matters too, and not only in the malicious sense. In practice, many incidents start with ordinary behaviour: emailing the wrong attachment, storing files in a personal drive, reusing credentials, or approving access without checking the role.
Legacy systems make both problems worse. Old applications often can't support modern authentication, granular access control, or reliable logging. Once they remain in production, they turn into a tolerated risk.
The blind spot called Shadow AI
One of the least discussed problems in healthcare data security is Shadow AI. A recent analysis noted that clinicians using unapproved public AI tools such as ChatGPT can send sensitive patient information to foreign servers, bypass institutional controls, and create a privacy compliance gap that many security frameworks still ignore (The Conversation on Shadow AI in Canadian digital health).
This happens for a simple reason. Public AI tools are fast. A nurse may want help rewriting notes. A physician may want a summary drafted. An administrator may want a letter cleaned up. If approved, internal tools are clunky or unavailable, staff will often solve the problem themselves.
That creates several risks at once:
Data leaves approved systems: Patient details may move outside your monitored environment.
Audit trails disappear: Security teams often can't see what was pasted, when, or by whom.
Jurisdiction becomes unclear: Data may be processed or stored outside Canada.
Policy lags behaviour: Many organisations ban unauthorised sharing generally, but don't state AI-specific rules.
Public AI use with patient data is often treated like a productivity issue. It's actually a data handling issue.
A broader discussion of sector-wide pressures appears in this overview of the importance of cybersecurity in the healthcare industry, but the practical takeaway is narrower: if your audit checklist doesn't ask where staff use AI, your security review is incomplete.
What to do about hidden use
You don't fix Shadow AI with a memo alone. You need a combination of controls:
Create an approved AI policy: Name what tools are allowed, what data may never be entered, and who approves exceptions.
Provide a safe alternative: If staff need summarisation or drafting support, offer a managed tool rather than only a prohibition.
Add AI to audits: Ask directly about browser tools, plugins, copied text, and documentation workflows.
Train on real examples: Staff respond better to concrete scenarios than abstract warnings.
The hidden danger in modern healthcare data security isn't only the attacker outside your network. It's the ungoverned shortcut inside it.
Navigating the Regulatory Maze in Canada and Beyond
Compliance in healthcare usually gets discussed in legal language. Clinic leaders need it in operational language. The practical test is straightforward: did you collect data lawfully, protect it reasonably, limit access appropriately, and handle incidents in a way regulators and patients can understand?
In Canada, that means paying close attention to federal and provincial privacy obligations. If you serve patients across borders, use foreign vendors, or process data for organisations outside Canada, other frameworks can become relevant too. HIPAA may matter if you touch U.S. healthcare workflows. GDPR can matter if personal data from Europe enters your environment. The details differ, but the leadership questions are similar.
The principles that matter in practice
Instead of memorising statutes, work from these decision rules:
Consent has to be meaningful: Staff shouldn't repurpose patient data casually because a system technically allows it.
Security has to be reasonable: “We trusted the vendor” won't satisfy scrutiny after an incident.
Access has to be limited: If everyone can see everything, your controls are weak, even if your software is expensive.
Patients have rights: Your systems and processes have to support access, correction, and accountable handling.
What LifeLabs made impossible to ignore
The clearest Canadian warning remains the LifeLabs breach. In December 2019, the company experienced a cyber-attack that exposed the records of potentially 15 million patients, and the company ultimately made a ransom payment, raising serious questions about prevention and accountability in Canada's healthcare security framework.
That case matters because it shows how failure spreads beyond one technical event. Once an organisation loses control of patient records at that scale, the consequences become regulatory, legal, reputational, and operational all at once.
Key judgement: Regulators don't only look at the breach. They look at the decisions that made the breach easier to cause, harder to detect, and slower to contain.
Compliance includes the end of asset life
A surprising amount of compliance risk sits in old equipment. Devices that still contain records, cached credentials, scans, or exported reports can create exposure long after they stop being useful. For hospitals and care facilities reviewing disposal procedures, this guide to Boston hospital IT asset disposition services is a practical example of the controls organisations should expect around the chain of custody, destruction, and documentation.
Teams building or updating regulated platforms also need software decisions mapped to privacy obligations from the start. That's where structured planning around healthcare compliance software development becomes useful, especially when consent, access logging, and retention rules have to be built into the product rather than bolted on later.
Building Your Digital Fortress Core Security Controls
A single stolen login can expose scheduling systems, billing records, lab results, and internal email within minutes. That is why core controls matter. In healthcare, they protect patient care as much as patient data.
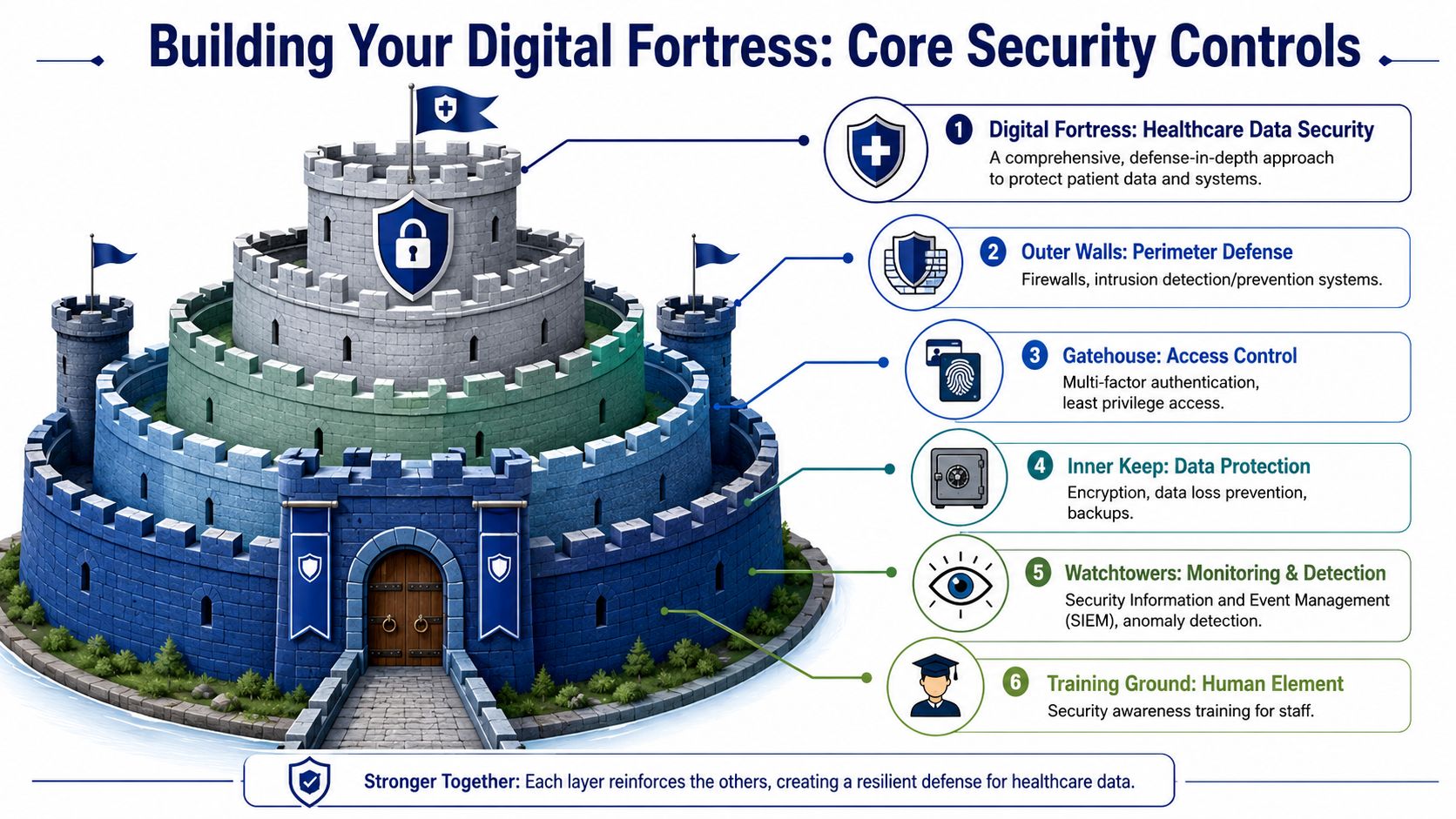
Outer walls and gatekeepers
Start with identity. If attackers can sign in as a real user, every downstream control gets harder to enforce.
Multi-factor authentication should cover email, remote access, administrator accounts, cloud consoles, and any application that stores or displays patient information. In practice, email is often the first priority because a compromised inbox can reset other accounts, approve fraudulent requests, and expose messages that contain sensitive data.
Least-privilege access comes next. Reception staff, clinicians, billing teams, contractors, and IT support do not need the same access. Shared accounts make investigations harder and misuse easier. Temporary access should expire automatically, and access reviews should happen often enough to catch role changes before they become security gaps.
Network segmentation reduces the blast radius. Clinical devices, finance systems, guest Wi-Fi, building systems, and back-office applications should not sit on one flat network. Segmentation does add administrative overhead. It also limits how far ransomware or a compromised device can spread.
The inner keep
Protection at the data layer needs to assume that perimeter controls will fail at some point.
A practical baseline includes:
Encryption at rest so stolen devices, copied databases, or exposed storage do not hand over readable records immediately
Encryption in transit, so data moving between users, clinics, labs, and cloud services is protected from interception
Immutable or isolated backups so ransomware cannot encrypt production and recovery copies in the same attack
Data minimisation so teams stop storing exports, duplicate files, and old records that no longer serve care, legal, or operational needs
Encryption helps, but it does not answer every risk. Canadian clinics using U.S.-based cloud platforms still need to decide where data is stored, which support teams can access it, and what legal exposure comes with foreign jurisdiction. I regularly see teams assume encryption settles the issue. It does not. Keys, admin access, backup locations, support workflows, and contract language all matter.
The same applies to Shadow AI. Staff paste referral notes, draft letters, insurance details, or patient questions into public AI tools because it is fast and easy. If that data leaves approved systems, encryption on your main platform does nothing to stop the disclosure. Core controls now need approved AI use policies, browser restrictions where appropriate, DLP rules for sensitive text, and training that gives staff a safe alternative instead of a blanket ban they will ignore.
The watchtowers
Many organisations buy security products before they build visibility. That order creates blind spots.
Focus on monitoring that answers basic operational questions. Who logged in, from where, what changed, what was exported, and what device was involved? If your team cannot answer those questions quickly, incident response slows down, and small events become larger ones.
Use these controls first:
Centralised logging for identity systems, endpoints, servers, firewalls, EHR access, and cloud administration events
Alerting for abnormal behaviour such as large exports, impossible travel, repeated failed logins, after-hours administrator activity, or disabled security settings
Modern endpoint protection with monitoring and response capability, not antivirus, left on default settings
Regular audit review so suspicious activity gets investigated before it becomes a reportable incident
If you cannot reconstruct an incident from your logs, you do not have monitoring. You have retained noise.
The training ground
Staff behaviour belongs in the control stack because real clinical work creates real shortcuts. Annual slide decks rarely change that.
Training should match the work people do. Front-desk staff handle identity verification and appointment messages. Clinicians use mobile devices, patient portals, and dictation tools. Billing teams send documents outside the organisation. Each group needs short, role-specific guidance tied to the decisions they make every day.
Include modern risk scenarios, not just phishing examples. Staff should know when AI tools are prohibited, when an approved tool can be used, how to avoid pasting PHI into public services, how to verify urgent payment or record requests, and how to report mistakes early. Early reporting matters because a ten-minute response is very different from a two-day response.
For organisations building healthcare products or custom integrations, one option in this space is Cleffex Digital Ltd, which provides software development services for healthcare workflows with attention to compliant handling requirements. That matters when access controls, audit trails, consent handling, and secure data flows need to be built into portals, apps, and integrations rather than added later.
A workable control order
If your organisation is behind, set the order based on risk reduction, not on which framework looks best in a board deck.
Lock down identity: MFA, shared-account removal, account cleanup, and role-based access.
Protect the data stores that matter most: Encryption, backup isolation, retention limits, and control over exports.
Reduce lateral movement and improve detection: Segmentation, central logging, endpoint monitoring, and useful alerts.
Set rules for real workflow risks: Shadow AI, remote access, messaging, printing, and local file storage.
Check the systems around your systems: Vendor access, support channels, and device lifecycle controls.
That sequence will not cover every edge case. It will close the failures that attackers and careless insiders use first.
Your Practical Security Roadmap by Organisation Size
A startup clinic platform, a ten-person family practice, and a regional healthcare enterprise don't need the same security programme on day one. They do need the same discipline. Start with the controls that match your exposure, your budget, and how your team operates.
One lesson applies across all sizes. In 2025, Anne Arundel Dermatology confirmed a breach affecting over 1.9 million patients, underscoring that even large organisations remain vulnerable and that basics such as multifactor authentication and encryption aren't optional (Falcon Systems on the Anne Arundel Dermatology breach).
Security Priorities by Organisation Size
| Priority Area | Healthcare Startup | Small Clinic (<10 Staff) | Medium Enterprise (10-500 Staff) |
|---|---|---|---|
| Identity and access | Build role-based access from the start. Avoid shared admin accounts. Turn on MFA everywhere. | Remove shared logins for front desk and billing. Review who still has access after staff changes. | Formalise IAM with approval workflows, privileged access controls, and recurring access reviews. |
| Data handling | Map where patient data enters the product, where it is stored, and which integrations touch it. | Stop ad hoc file storage. Keep records in approved systems only. Control exports to spreadsheets and local drives. | Classify data, restrict high-risk exports, and align retention with legal and operational needs. |
| Monitoring and response | Use managed logging and basic alerting early. Start with visibility, not tool sprawl. | Ensure someone reviews alerts and backups. A tool without an owner won't help. | Build incident playbooks, escalation paths, legal coordination, and vendor response procedures. |
What a startup should do first
Early-stage healthcare companies often make one dangerous assumption: because the team is small and trusted, access can stay informal. That usually leads to over-privileged accounts, production data copied into test environments, and no clean boundary between development and operations.
The smarter approach is to build guardrails early:
Use separate environments: Don't let developers use live patient data casually.
Review cloud defaults: Many breaches begin with weak configuration, not exotic attacks.
Approve AI use before launch pressure rises: Once the team normalises public tool use, it's hard to pull back.
What a small clinic should do first
Small clinics usually don't fail because of advanced attackers. They fail because no one owns the details. Password sharing becomes normal. Old laptops sit in cupboards. Remote access stays enabled for former vendors. Staff forward documents because it's fast.
The highest-value moves are operational:
Assign a named security owner, even if security isn't their full-time role.
Document approved tools for email, messaging, storage, and chart access.
Run a device and account cleanup every time staffing changes.
Test backup restoration, not just backup completion notices.
Small teams don't need a huge programme. They need fewer exceptions.
What a medium enterprise should do first
At this size, the risk shifts from “do we have controls?” to “are controls consistent across departments, sites, and vendors?” Security often becomes uneven. One department has strong onboarding and logging. Another uses legacy workflows nobody wants to disturb.
Medium organisations should tighten governance:
Standardise access reviews across business units
Map vendor dependencies and integration points
Add a formal risk assessment to change management
Create executive-level incident decision paths
The roadmap that works is the one your organisation can operate every week, not the one that looks strongest in a policy binder.
Choosing Secure Partners and Managing Vendor Risk
A clinic can have solid internal controls and still expose patient data through a weak vendor. That is the practical reality of modern healthcare. Your EMR, billing platform, patient portal, transcription service, cloud backup, outsourced developer, and AI-enabled support tools all sit somewhere in the chain of custody.
Vendor risk is now patient risk.

Ask where the data actually lives
Canadian organisations often hear, "We serve Canadian clients," and stop there. That answer is too vague to be useful. Key questions are about residency, access, and legal exposure.
A vendor may offer a Canadian-facing service while storing production data, backups, logs, or AI processing outputs in the United States. That matters for two reasons. First, it changes which laws and disclosure regimes may apply to your patient data. Second, it can complicate breach response, audit rights, and patient notification decisions.
At this point, data sovereignty stops being a policy discussion and becomes an operational one.
Ask direct questions:
Where is production data stored
Where are backups and disaster recovery copies stored
Which countries can vendor staff access data from
Which subprocessors handle hosting, support, analytics, or AI features
Whether customer data is used to train any AI model, directly or indirectly
How data is returned, deleted, and verified at contract end
That AI question needs special attention. Shadow AI is not only an internal staff problem. Vendors now add AI features discreetly into transcription, summarisation, support chat, scheduling, and analytics workflows. If a supplier cannot explain how patient data is isolated from model training, where prompts are processed, and how outputs are logged, do not assume the risk is acceptable.
The vendor checks that prevent expensive surprises
Good vendor review does not require a large procurement office. It requires discipline. The goal is to confirm how the vendor operates before an incident forces you to find out the hard way.
Focus on the contract first. Security promises made in sales calls do not help much if they are not written into the agreement.
Contract and control checks
Security obligations: Define access control, encryption expectations, incident notification timeframes, audit support, and secure deletion requirements.
Logging and evidence: Confirm what audit logs exist, how long they are retained, and whether you can get them quickly during an investigation.
Subprocessor visibility: Require a current list of subprocessors and notice of material changes.
Data use limits: State clearly that patient data cannot be used for model training, product improvement, or testing unless that use has been explicitly approved.
Residency commitments: If Canadian data residency matters to your organisation, put it in the contract. Do not leave it as a sales assurance.
Operational checks
Breach coordination: Confirm who contacts whom, how fast, and what details the vendor must provide.
Change management: Ask how major platform changes, new integrations, or new AI features are reviewed and communicated.
Access handling: Check how vendor staff access production systems, whether sessions are logged, and how privileged access is approved.
Exit plan: Make sure you can export data in a usable format and verify deletion afterwards.
Teams that want a repeatable intake process often benefit from a documented software vendor onboarding roadmap so security, privacy, legal, and operations can review the same risks in the same order.
What good partner selection looks like
Good partner selection is slower at the start and less painful later. In practice, that means declining tools that are convenient but opaque, pushing back on vague answers, and accepting that some low-cost platforms create high-cost exposure.
I advise clinic leaders to treat vendor review as a business decision with security consequences, not as a procurement formality. If a supplier cannot answer clear questions about residency, subcontractors, AI data handling, logging, or deletion, the problem is not your questionnaire. The problem is the vendor.
For Canadian healthcare organisations, this issue has become sharper. Many widely used cloud services are operated by U.S.-based companies, even when the product is marketed locally. That does not make every U.S.-linked vendor unacceptable. It does mean you need to choose deliberately, document the trade-offs, and know exactly whose laws, infrastructure, and staff sit between your patients and their data.
What to Do When a Breach Happens: An Incident Response Plan
When a breach happens, the first mistake is improvisation. The second is letting technical staff handle everything without legal, operational, and leadership input. A workable incident response plan keeps people calm because it gives them sequence and authority.

The first moves
Treat the first day as a control exercise, not a forensic debate.
Detect and verify
Confirm what triggered the concern. Was it suspicious login activity, unusual exports, malware alerts, unavailable systems, or vendor notification?Contain
Isolate affected accounts, devices, applications, or network segments. If necessary, disable access fast and accept short-term disruption.Preserve evidence
Don't start wiping systems blindly. Capture logs, account activity, system states, and vendor communications.
Who needs to be involved
A healthcare breach is never only a technical event. The response team should include:
Executive decision-makers: So containment and communications aren't delayed
IT or security leads: To manage technical triage
Privacy and legal advisors: To assess notification duties and regulatory exposure
Operational leads: To keep patient services running safely
Communications support: If patients, partners, or media must be informed
Recovery and notification
Once the immediate threat is contained, move carefully. Restore systems in a controlled order. Validate integrity before reopening broad access. Review whether any workaround created a new risk.
Canadian organisations also need to assess reporting and notification duties under applicable privacy law. That means documenting what happened, what information was involved, who may be affected, what harm could result, and what mitigation steps are being taken.
The right response plan doesn't try to prevent stress. It prevents confusion.
After recovery, run a disciplined review. Identify the entry point, the failed control, the delayed decision, and the policy gap. If Shadow AI, weak vendor oversight, or poor access management contributed, update the operating model, not just the incident report.
If your organisation needs secure healthcare software, cloud-aware architecture, or compliance-conscious product development, Cleffex Digital Ltd is one option to evaluate. As a Canada-based software development company, Cleffex works on digital solutions for healthcare and other regulated environments where security, integration, and operational reliability need to be built into the product from the start.







