



Many healthcare products start the same way. A clinic lead, founder, or operations manager sees a real bottleneck every day: referrals trapped in inboxes, intake forms re-entered by staff, follow-up gaps that frustrate patients, or insurance workflows that waste clinician time. The product idea is usually sound. The trap is assuming the hard part is building screens and shipping an app.
In Canada, the hard part is building something that can survive contact with clinical workflow, privacy obligations, procurement reality, and fragmented provincial systems. That’s where many teams stall. They have a good concept, maybe even a prototype, but no practical path to turn it into a dependable healthcare product.
That’s what healthcare product engineering services are for when they’re done properly. Not outsourced coding. Not a generic dev shop with a healthcare page. A disciplined partnership that can take a health product from concept to validated release, without creating technical debt, compliance exposure, or integration problems you’ll be paying for later.
The Digital Health Idea and the Engineering Gap
A common Canadian scenario looks like this. A small clinic group wants a patient-facing mobile app tied to scheduling, secure messaging, reminders, insurance workflows, and access to care plans. The business case feels obvious. Staff are overloaded, patients expect digital access, and leadership wants something more useful than another disconnected portal.
Then reality lands.
The clinic needs the app to work with an existing EMR, a billing process that was never designed for APIs, and regional data expectations that differ depending on where the clinic operates. Someone asks about consent handling. Someone else asks whether the messaging function becomes part of the medical record. Then the insurer workflow enters the discussion, and nobody can agree on what data should move automatically and what needs human review.
Why Good Ideas Stall
Teams often don’t fail because the idea is weak. They fail because they underestimate the engineering gap between an idea and a clinical product.
That gap usually includes:
Clinical workflow ambiguity that sounds minor early on but breaks adoption later
Data design mistakes, such as storing patient, encounter, and billing data in ways that don’t support auditability
Security shortcuts like broad user permissions or weak logging
Integration assumptions based on vendor promises instead of tested interfaces
Procurement drift, where the scope expands faster than the budget, and decisions stop being tied to outcomes
A generic software partner often treats these as implementation details. In healthcare, they are product-defining decisions.
Practical rule: If a partner starts with wireframes before mapping data flows, roles, risk, and system boundaries, they’re building a demo, not a healthcare product.
What the Right Partnership Changes
A seasoned engineering partner brings structure where internal teams usually have uncertainty. They force early decisions on what the product is, who it serves first, which workflows matter, what must be integrated now, and what can wait.
That changes the project in practical ways:
The first release gets smaller and sharper. You stop trying to solve every clinic pain point at once.
Architecture reflects regulation and operations. Audit trails, permission models, and data retention aren’t bolted on later.
Integration work is treated as a primary workstream. It gets budget, testing time, and fallback plans.
That’s the primary function of healthcare product engineering services. They bridge the space between a medical or operational idea and a product that users can trust, buyers can approve, and teams can maintain.
Defining Healthcare Product Engineering
Healthcare product engineering isn’t ordinary software development with medical terminology added on top. It’s the full discipline of designing, building, validating, launching, and evolving a digital health product in an environment where patient safety, traceability, and operational fit matter as much as features.
A useful analogy is the difference between fitting out an office and building an operating theatre. Both involve construction. Only one requires specialised airflow rules, controlled access, equipment integration, documented procedures, and zero tolerance for avoidable failure. Healthcare software is closer to the second category.
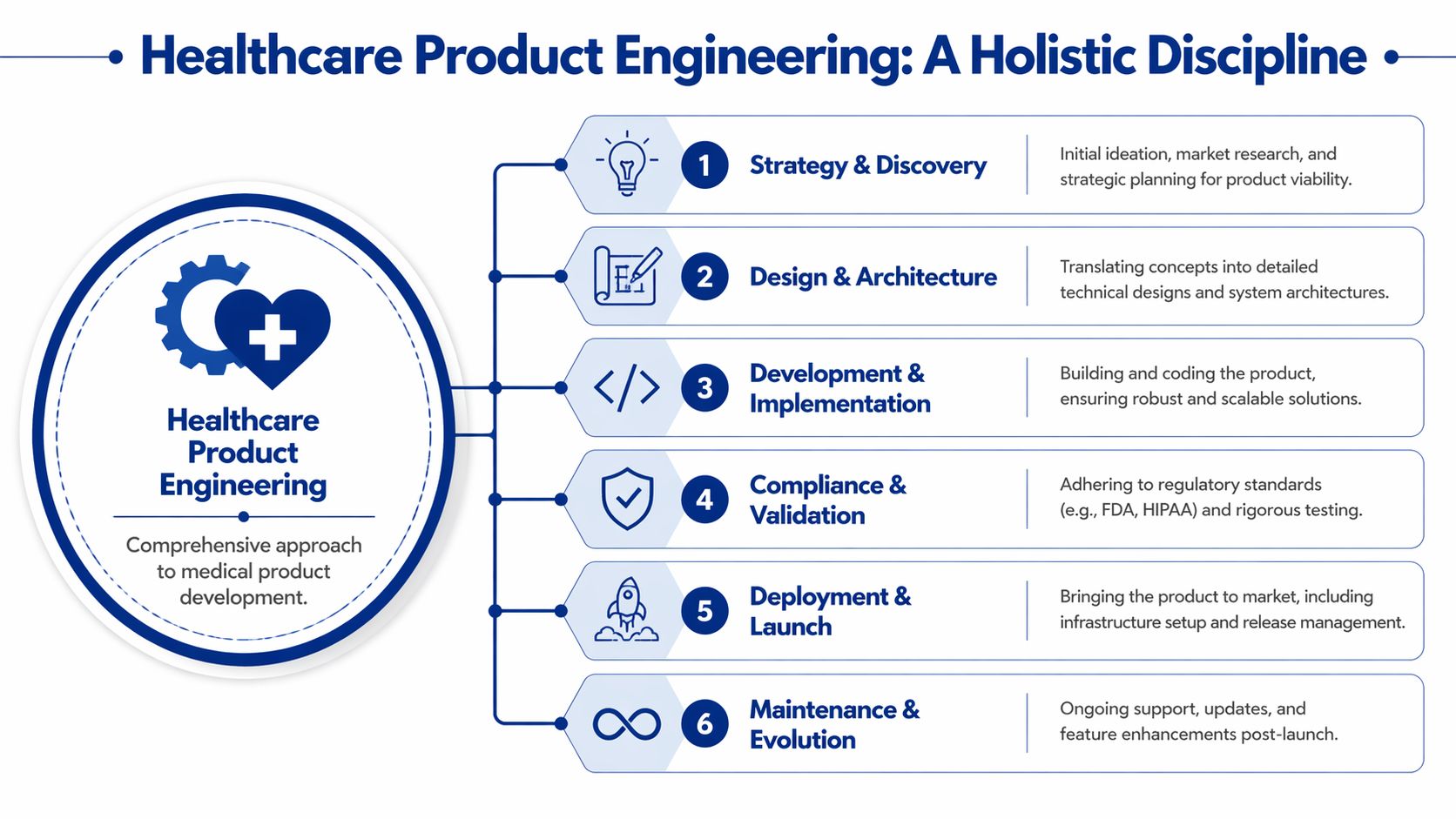
It Covers the Full Product Lifecycle
When teams buy healthcare product engineering services, they should expect capability across the lifecycle, not just sprint delivery.
That usually includes:
Discovery and product framing so the team knows which problem is worth solving first
System architecture that defines data boundaries, integrations, hosting, and failure handling
UX design for clinical and patient use with attention to interruptions, mobile contexts, and accessibility
Implementation and integration across app layers, APIs, third-party systems, and operational tooling
Verification and validation with rigorous QA, traceability, and release discipline
Post-launch maintenance that treats support, monitoring, and controlled change as part of the product
This is why a healthcare build often needs a broader bench than founders expect. You don’t just need developers. You need product thinkers, architects, QA leads, security input, and people who know how regulated workflows behave in production.
How It Differs From General Outsourcing
Generic outsourcing focuses on task completion. Healthcare engineering focuses on decision quality.
A general-purpose team might say, “We can build that feature.” A healthcare-capable team asks different questions first:
Should that feature exist at all in the first release?
What clinical or operational action does it trigger?
Does it create record-keeping obligations?
What happens if the third-party system is unavailable?
How will a clinic prove what happened if there’s a dispute?
Those questions save projects.
For teams evaluating specialist vendors, it’s useful to look at adjacent disciplines too. If your roadmap extends into regulated devices or connected diagnostics, a guide to medical device engineering services helps clarify where software engineering ends and device-grade engineering expectations begin.
The Outcome Is Not Just Software
The deliverable isn’t “an app”. It’s a controlled product system. That means code, yes, but also data rules, test evidence, deployment procedures, access control, monitoring, support workflows, and a roadmap that can evolve without destabilising the product.
If you want a broader view of how this differs from ordinary custom builds, Cleffex’s discussion of healthcare software development is useful because it highlights the operational and compliance layers that standard software teams often miss.
The fastest team is rarely the one that writes code first. It’s the one that reduces rework by making the right architectural and regulatory decisions early.
Core Capabilities Your Product Cannot Live Without
A healthcare product can look polished and still be structurally weak. I’ve seen teams spend months refining dashboards while leaving authentication brittle, integration assumptions untested, and audit logging incomplete. In healthcare, those are not secondary defects. They are product risks.
The essential capabilities sit underneath the visible experience. If your partner is weak in these areas, the roadmap eventually slows, the compliance burden rises, and the cost of every change goes up.
Secure Architecture and Data Boundaries
The architecture has to reflect how healthcare data moves, who should see it, and how failures are contained. That sounds obvious, but many early products are built like ordinary SaaS tools. Broad admin roles. Shared data access patterns. Weak separation between clinical actions, messaging, billing events, and analytics.
A better architecture does a few things from the beginning:
Separates core data domains so patient identity, appointment data, clinical notes, and financial events aren’t all tangled together
Implements role-based access carefully rather than relying on a single “admin” concept
Logs sensitive actions, including record views, edits, exports, and integration events
Plans for failure states, such as delayed sync, duplicate records, and partial transactions
If this groundwork is missing, every later feature becomes slower and riskier to ship.
Cybersecurity That Fits Healthcare Reality
Security in healthcare isn’t just about keeping attackers out. It’s also about preventing legitimate users from making unsafe or non-compliant mistakes.
That’s why strong engineering partners build security into daily workflows:
Least-privilege access so staff only see what they need
Encryption in transit and at rest as a baseline, not an upgrade
Session and device controls for mobile and distributed teams
Structured audit trails for investigations, disputes, and compliance review
Secure SDLC practices, including code review, dependency management, and release gates
A product can pass a feature demo and still be unready for a real clinic if these controls are immature.
Interoperability in the Canadian Context
Many imported playbooks break down. Canadian healthcare isn’t one system. It’s a set of provincial and territorial realities with different processes, vendors, and data expectations.
A 2025 CIHI report noted that only 28% of Canadian primary care providers have achieved meaningful EHR interoperability across provinces, and a 2024 Ontario Health study found that 65% of small clinics cite integration costs with provincial data silos as the top barrier to adopting new technology. For small clinics and startups, that changes engineering priorities immediately.
You can’t treat interoperability as a nice-to-have backlog item. In Canada, it often determines whether the product is usable at all.
What Competent Interoperability Work Looks Like
A credible partner should be comfortable with standards such as HL7 and FHIR, but standards knowledge alone isn’t enough. The practical work is messier.
Look for teams that can handle:
API mediation and middleware layers when the source system can’t expose clean, modern interfaces
Mapping and transformation logic between inconsistent schemas
Identity reconciliation when patient records don’t line up cleanly across systems
Queueing and retry strategies so failed exchanges don’t corrupt workflows undetected
Version-tolerant integration design because upstream systems change on their own schedule
If a vendor says “FHIR solves interoperability,” they haven’t spent enough time integrating healthcare systems.
QA and Validation That Go Beyond Bug Counts
Healthcare QA isn’t just regression testing and UI checks. It includes scenario design for clinical edge cases, permission testing, integration reliability, and evidence that changes behave as intended.
A mature validation approach often includes a mix of:
Risk-based test planning tied to what could cause patient harm, workflow disruption, or record errors
End-to-end integration testing across the product and the external systems it depends on
Negative testing for incomplete forms, interrupted sessions, duplicate submissions, and unexpected user behaviour
Release evidence that proves what was tested, what changed, and what remains constrained
That discipline feels slower in the short term. It’s much faster than recovering from avoidable production failures.
The Next Frontier: AI Cloud and DevOps in MedTech
AI, cloud, and DevOps used to sit in the “advanced roadmap” category. For most healthcare products now, they’re baseline capabilities. Not because every product needs a flashy AI layer, but because modern products need scalable infrastructure, reliable release processes, and a realistic plan for using automation without stepping into regulatory trouble.
The market pressure is simple. Buyers want faster implementation, better user experience, cleaner automation, and ongoing improvement. You can’t meet that with brittle hosting, manual deployments, and ungoverned model behaviour.
AI Without Compliance Discipline Is a Launch Risk
A lot of teams still treat AI as a prototyping shortcut. They build a classification flow, triage assistant, documentation helper, or patient interaction layer, and assume compliance can be tidied up later. In Canada, that’s a weak bet.
Canada's proposed Artificial Intelligence and Data Act requires risk-tiered audits for healthcare AI, and a January 2026 Health Canada survey found that 55% of startups lack engineering partners versed in AIDA's compliance tools, leading to significant launch delays and higher rejection rates.
That has a direct implication for vendor choice. If your product uses AI in any meaningful clinical, operational, or patient-facing flow, the engineering partner must know how to build traceability, model governance, risk controls, and validation evidence into the product itself.
Where Teams Get AI Wrong
The common failures are predictable:
They prototype before defining the intended use
They skip auditability for prompts, outputs, and overrides
They blur assistive and decision-driving behaviour
They don’t design fallback workflows for uncertain model output
They treat model updates like ordinary feature releases
Those mistakes don’t just create legal exposure. They make products hard to defend during procurement and hard to trust in practice.
For teams considering patient interaction tooling, it helps to review implementation patterns in Conversational AI for Healthcare. The useful takeaway isn’t hype. It’s that conversational interfaces only work in healthcare when the handoff rules, escalation logic, and documentation boundaries are engineered properly.
Cloud Is the Operating Model
Healthcare teams still occasionally ask whether the cloud is optional. In practice, cloud is the operating model for products that need resilient environments, controlled access, observability, and scalable delivery across locations and teams.
That doesn’t mean “move everything fast”. It means engineering the right workloads in the right way.
A sensible cloud approach usually includes:
Environment separation for development, test, staging, and production
Infrastructure as code, so environments are reproducible and reviewable
Centralised logging and monitoring across apps, APIs, jobs, and integrations
Managed services where appropriate to reduce operational fragility
Backup and recovery planning that aligns with product criticality
In healthcare, cloud architecture is not just a hosting decision. It’s part of your risk posture.
If you want a practical view of how release automation and infrastructure discipline fit together, this overview of cloud DevOps software delivery is a good companion read.
DevOps Is How Safe Products Evolve
Healthcare products don’t stand still after launch. Payers change requirements. clinics ask for workflow changes. integrations break. browsers update. operating systems shift. A team without DevOps maturity ends up treating every release as a stressful mini-migration.
A strong DevOps practice reduces that chaos through repeatable pipelines, release controls, automated testing, environment consistency, and rollback discipline.
Good DevOps in medtech doesn’t mean shipping recklessly. It means changing the system often enough that no single release becomes dangerous.
That’s why AI, cloud, and DevOps belong together in healthcare product engineering services. They are the practical foundation for products that need to improve continuously while staying governable.
Choosing Your Engineering Partner Wisely
Most buyer mistakes happen before a single line of code is written. Teams evaluate partners on presentation quality, daily rates, or a polished demo environment. Then they discover the vendor has weak clinical instincts, no opinion on Canadian interoperability, or a project model that hides risk until late.
The stronger way to choose is to assess strategic fit across three dimensions at the same time: domain judgement, delivery maturity, and working relationship. Miss any one of those and the engagement gets expensive.
Domain Judgement Matters More Than Slide Decks
A competent partner should be able to discuss your product in operational terms, not just technical ones. They should ask how staff currently work, where patient risk could be introduced, what needs to become part of the record, and which integration points can block adoption.
Ask them to walk through a realistic scenario. Not a generic user journey. A specific one. A patient updates intake information, a staff member reviews it, something conflicts with an existing record, and an insurer-related field doesn’t map cleanly. Listen to how they think.
Good partners talk about exception handling, reconciliation, permissions, and traceability. Weak ones jump back to UI polish.
Delivery Maturity Shows Up in Unglamorous Answers
You learn more from a vendor’s answer about failed sync jobs, test evidence, and release rollback than from any claims about innovation.
Use questions like these:
How do you document assumptions in discovery so the scope doesn’t drift unchecked?
What artefacts do you produce before development starts?
How do you test external integrations that are unstable or poorly documented?
What does release approval look like for a healthcare product?
How do you handle audit trails and access reviews?
A serious partner won’t answer with slogans. They’ll describe a working method.
When a vendor can explain how they recover from ambiguity, outages, and changing requirements, you’re hearing the truth about how they operate.
Cultural Fit Is Not a Soft Issue
Healthcare projects create pressure. Stakeholders disagree. Clinical users request changes late. Procurement slows decisions. Regulations shape architecture in ways non-technical leaders don’t always understand. A partner who communicates poorly will magnify every one of those problems.
Look for evidence that they can operate as an extension of your team:
They challenge assumptions respectfully
They surface risks early, even when the news is unwelcome
They can work with clinical and non-technical stakeholders
They write clearly
They don’t hide behind ticket systems when decisions need escalation
What Long-Term Value Actually Looks Like
The best partner is not the cheapest team or the biggest brand. It’s the one that helps you make durable product decisions, preserve optionality, and avoid rebuilding core parts of the system after launch.
That’s why evaluation should include present needs and future paths. If the product later adds AI features, broader integrations, device connectivity, or insurer-facing workflows, can this team support that evolution without forcing a rewrite?
If the answer is uncertain, keep looking.
Engagement Models and Pricing Demystified
The wrong engagement model can sink a good project. I’ve seen fixed-price contracts applied to discovery-heavy products, which turns every new learning into a change request battle. I’ve also seen open-ended time and materials used on poorly defined teams, which creates endless motion with little accountability.
The model should match the uncertainty in the product, not just your procurement preference.
The Three Models Most Teams Consider
Here’s a practical comparison.
| Model | Best For | Pros | Cons |
|---|---|---|---|
| Fixed Price | Narrow, well-defined scopes with stable requirements | Predictable commercial structure, easier internal approval, clear deliverables | Weak fit for evolving products, change requests pile up, vendors may optimise for contract protection over product quality |
| Time and Materials | Discovery-heavy products, evolving feature sets, integration work with unknowns | Flexible, supports iteration, better for learning during the build | Needs strong governance, budget can drift, weak product ownership creates waste |
| Dedicated Team | Multi-phase products, ongoing platforms, long-term roadmap execution | Team continuity, deeper product knowledge, stronger collaboration, better for scale and maintenance | Requires active client involvement, not ideal for very small one-off builds, commitment feels heavier early on |
How To Choose Without Fooling Yourself
If your requirements are still moving, your integrations aren’t fully understood, or your compliance boundaries are not settled, a fixed price usually looks safer than it is. It only feels predictable because uncertainty is being hidden in assumptions.
A more realistic mapping is:
Choose Fixed Price when the scope is small, bounded, and the acceptance criteria are easy to define
Choose Time and Materials when discovery is part of the work, and you need room to adapt
Choose a Dedicated Team when the product is becoming a long-term capability, not a project
The hidden issue is governance. Flexible models work well only when the client can make decisions, review progress, and prioritise trade-offs quickly.
What Actually Drives Cost
Healthcare product engineering services are priced by more than developer hours. Cost tends to move with the complexity of the problem.
The biggest drivers are usually:
Integration burden, including legacy systems, APIs, middleware, and test environments
Risk and compliance needs such as validation evidence, auditability, and security depth
Workflow complexity across staff, patients, insurers, and administrators
Release expectations, including environments, automation, support, and monitoring
Team composition, because senior architecture and QA capability often matter more than raw coding capacity
If you’re comparing commercial structures across vendors, it helps to explore various pricing models elsewhere too, to sharpen your sense of how pricing logic changes with scope, support, and product maturity.
A Practical Buying Rule
Don’t ask vendors for the cheapest number. Ask for the clearest commercial logic.
A healthy proposal explains what’s included, what assumptions the estimate depends on, what could force reprioritisation, and how governance will work if the product changes. That kind of transparency is more valuable than a low headline figure.
Your Actionable Procurement and Risk Mitigation Checklist
Once you decide to engage an external partner, the first month matters more than is commonly understood. The initial phase determines whether you establish control or inherit avoidable risk. Procurement shouldn’t start with legal redlines. It should start with a disciplined operating plan.
Days One to Ten on Problem Framing and Evidence
Before you ask for a detailed proposal, tighten the product brief. Not the pitch deck. The operating brief.
Include:
Primary user and workflow with one clear release priority
System context covering current software, data sources, and external dependencies
Constraints such as privacy expectations, insurer workflow rules, and internal approval realities
Success criteria framed as operational outcomes, not feature volume
Known unknowns so vendors can estimate accurately
At the same time, verify the partner’s evidence. Ask for examples of healthcare delivery, integration-heavy work, and regulated or compliance-sensitive releases. Don’t just review screenshots. Ask what went wrong in those projects and how the team handled it.
Days Ten to Twenty on Technical and Compliance Diligence
Many buyers often stay at a high level. Go lower.
Review these areas directly:
Security controls
Ask how access is managed, how secrets are handled, how logging works, and how incidents are escalated.Architecture ownership
Confirm who makes system design decisions and what artefacts will be produced before implementation accelerates.Integration strategy
Ask how they test third-party dependencies, handle retries, reconcile mismatched records, and document interface assumptions.Quality model
Request their approach to regression, end-to-end testing, release sign-off, and defect triage in healthcare contexts.Compliance awareness
Make sure they can discuss Canadian healthcare privacy and software compliance in practical terms. This resource on healthcare compliance software development is useful as a benchmark for the kinds of controls and design considerations your questions should surface.
A partner who can’t explain their controls clearly before contracting won’t become clearer after the contract is signed.
Days Twenty to Thirty on Contract Protections
Your Statement of Work and Master Service Agreement need to protect continuity, clarity, and exit options. Don’t leave these buried in generic vendor templates.
Make sure the paperwork addresses:
Intellectual property ownership with no ambiguity around code, designs, documentation, and work product
Acceptance criteria tied to measurable deliverables, not vague completion language
Change management so that scope adjustments have a defined process
Documentation obligations covering architecture, environments, integrations, and operational runbooks
Confidentiality and data handling with explicit responsibilities
Exit and transition terms so another team can take over if needed
Support expectations for defects, incidents, and post-launch stabilisation
The Checklist To Use in Practice
Keep this short list in front of the team during procurement:
Define the first release narrowly
Map every critical data flow before building approval
Confirm who owns the architecture decisions
Test the vendor’s thinking on edge cases, not just happy paths
Require visibility into the QA and release process
Write transition rights into the contract
Treat integration work as a primary budget line
Document assumptions so surprises become explicit decisions
Procurement is not administration. In healthcare, it is part of product risk management.
Cleffex Digital Ltd helps organisations build secure, scalable digital products with agile delivery and practical engineering depth. If you’re planning a healthcare platform, modernising a clinic workflow, or shaping an AI-enabled product for the Canadian market, Cleffex Digital Ltd is worth considering as a development partner that understands how technology, compliance, and delivery discipline need to work together.







